Hi all, just received my machine yesterday. I was diagnosed 35+ AHI during sleep study. This is my first night on APAP! Please share your insight!! What numbers should I be looking at? What are some tips and suggestions you may have. Please point out any significance for me. Thank you in advance!
Welcome to the forum. Those results look pretty good for a first night. I would make a few small changes to the setup though. Here are some things to discuss with your provider about changing, unless you are adjusting your own machine.
You can post SleepyHead images here by simply left clicking on them, and dragging them into an open post that you are making. Hope that helps some, Post again if you need help or have more questions...
Welcome,
I on the other hand like to use EPR full time especially when I see the flow limits on your flow limit chart. I do not believe that it pushes your Inspiration pressure higher. BUT, as Sierra pointed out you have a fair amount of central apnea/clear airway events, not enough to worry about but enough to avoid.
EPR can treat hypopneas and flow limits which is a good thing but the pressure variation between inhale and exhale can, and frequently does, contribute to Central Apneas. My recommendation would be to reduce EPR to 1 and full time and observe and if the central apneas persist I would turn EPR Off to avoid the Central Apnea. And if that doesn't work to lower your max pressure for 2 reasons, reduce the variation which is known to bring out centrals and higher pressures are known to do the same thing.
It is not uncommon to have to go to a narrow band of pressure or a fixed pressure to find the right balance between avoiding the central apnea and treating your obstructive apnea.
Note: It is possible to lower the IPAP pressure by increasing the EPR and better managing the flow limitations which do trigger pressure raises. The only way to know for sure in your case would be to try it.
Fred
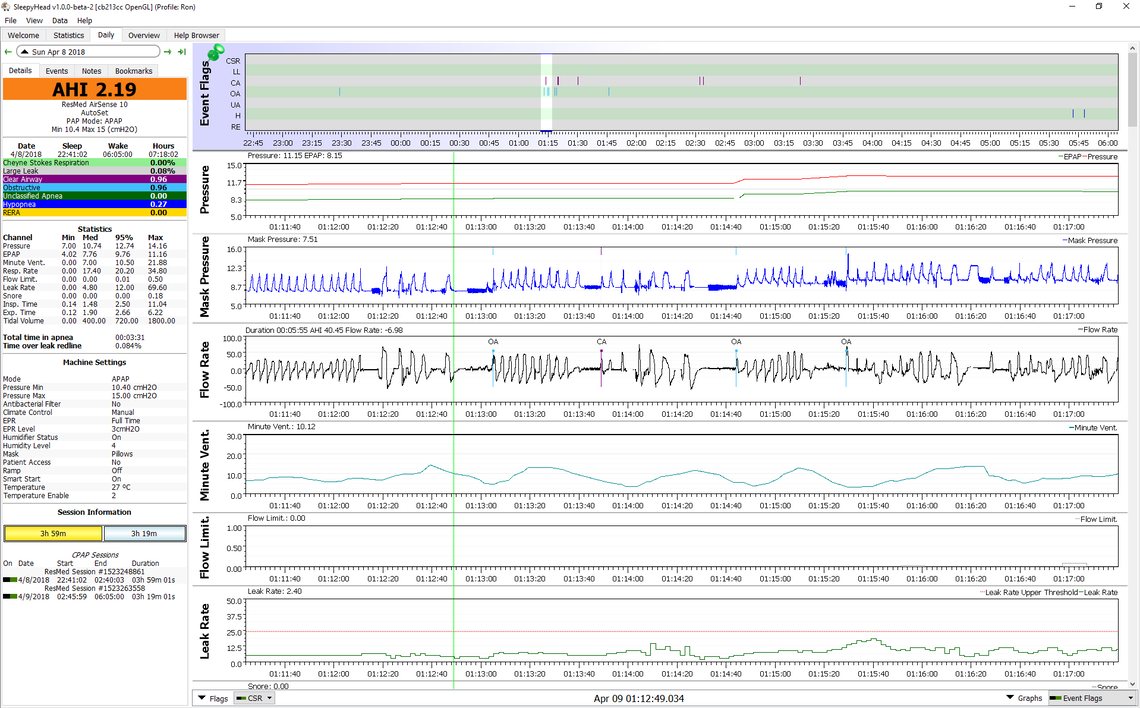
I would agree with one thing. That is that everybody is somewhat different. For example turning EPR to zero helps me more than it does my wife. Her apnea is essentially all obstructive. Mine is mixed central and obstructive. When I use EPR and look at events in SleepyHead what I see is that the obstructive apnea starts at the lower EPAP pressure. If you look at the screenshot below which was from April last year when I was using EPR at 3, the OA event starts at 7.5 cm of pressure. But it cycles up to 10.5 cm on inhale which does no good for the obstruction at the lower pressure. In fact what it does for someone that has pressure sensitive central apnea is create CA events. It is kind of the worst of both worlds. Low pressure causing OA, and high pressure causing CA. What I know now, that I am smarter about the stuff is that 10.5 to 11 cm is enough to prevent obstructive apnea for me. That is all I need on exhale. If I was to leave EPR at 3 turned on, I would need to endure 14 cm on IPAP. That would create more CA. For that reason my final solution has been to run a fixed CPAP pressure of 11 cm, with EPR on ramp only when you are awake and don't get apnea.
My wife gains about 1.5 cm of pressure by turning off EPR of 3, and I probably gain 2.5 cm, by turning it off.
I don't buy into the rules of thumb about treating hypopnea, because again everyone is different. The one thing you don't know (and the machine does not know either) is whether or not a hypopnea is due to a lack of breathing effort (central), or due to flow resistance (obstructive). For someone that has flow resistance due to impending obstructive events, more pressure helps and EPR may help some too. But for someone that has central hypopnea, more pressure hurts and EPR hurts too. That is the underlying reason why someone with mixed apnea (like the OP has a mild case of) needs to limit maximum pressure. The machine is not smart enough to stop raising pressure for central hypopneas. It just makes things worse instead of better.
To the OP, if you look at your EPAP pressure (green trace) for each OA event and record it, that will give you a pretty good idea what pressure you need to prevent OA events. You might need 1-2 cm above the highest one. Hard to read on your graph but that is probably in the order of about 11 cm -- the same as I use... When you are running a pressure above that you are likely increasing the frequency of CA events.
Sierra and Bonjour, thank you for replies. I look forward to posting my results again tomorrow morning and would like you all to continue the conversation. Since it is my first time of using this machine and reading the data, all of these medical vocabulary and terms are new to me and I have minimal clue how to interpret them.
For tonight, I will change EPR to 1 instead of 2, and just change min pressure to 7 and max to 14. Sierra, should I leave EPR full time? Why do I need auto ramp? I feel auto ramp is too slow at the beginning....I could handle the min pressure starting at 7 at the beginning and do not feel a thing. Any other suggestions I should do for tonight would be greatly appreciated :).
The secret of using the Auto Ramp is to set the Ramp Start pressure higher. I think 7 cm is the minimum for comfort, and it can be higher if your minimum pressure is higher. I currently have a ramp start at 9 cm. The Auto Ramp is not really a ramp. It simply holds the pressure at the Ramp Start Pressure setting until you go to sleep. So it is really a pressure hold. It also gives you the option to set the EPR Type to Ramp only. I would leave EPR at 3 and set it to Ramp only, once you have set the Ramp to Auto and the start pressure at 7. The EPR at 3 on Ramp Only will not increase your pressures during the night. It is essentially a comfort setting and for most people really only needed while they are awake.
What these settings will do is start you immediately at 7 cm on inhale and 4 cm on exhale. Most find that very comfortable. Then when you go to sleep the EPR reduction stops, and you get the 7 cm on inhale and exhale. The machine will then adjust that pressure based on apnea hypopnea events. Down the road you probably will want to increase that minimum pressure some. Having the minimum pressure higher avoids those events that trigger the pressure to increase in auto. You take a bit of control away from the machine, and start preventing events as soon as you fall asleep.
Another tip is that you can't base much on one night. I think your setting are a fair bit away from optimum now, so it doesn't hurt to make the changes suggested. However once you get closer to an optimum setting you will want to leave things alone for several nights to see what they do on average.
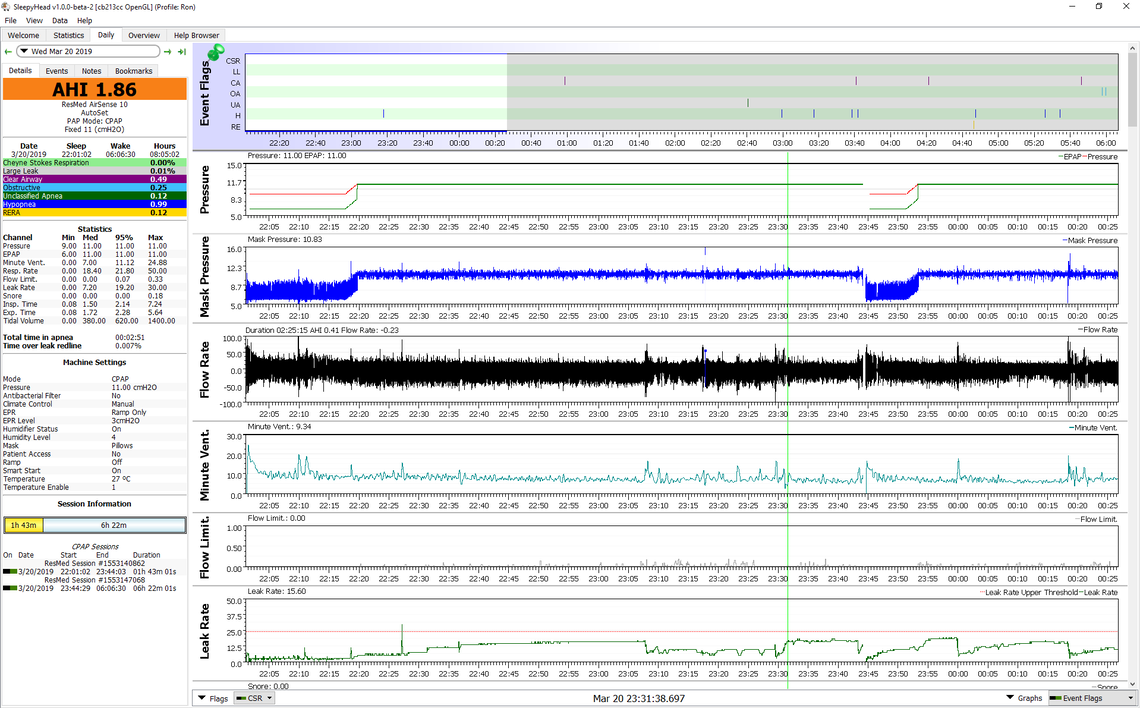
Edit: This is what an Auto Ramp, EPR 3, Ramp Only setup looks like in SleepyHead. You can see that the pressure just holds and cycles up and down with each inhale and exhale until you go to sleep, then there is a very short ramp up to the minimum pressure if minimum is higher than the ramp start. I am currently using a fixed pressure of 11 cm, so you don't see any fluctuation of pressure during the sleeping. The second Auto Ramp period was probably after my mask hose came disconnected. I've been having that issue lately. In any case you can see the ramp period is shorter as I went to sleep faster, then it ramped up again.