

Previously, I've been trying a typical combination of 7 minimum with a max of 9. While the ramp sometimes would go up to 10 if I set it to 10 or 11, I would also get more centrals when it did that. Keeping it lower seems to keep those centrals in check. 8.9 is known to be my sweet spot that the auto ramp always stops at when I'm decently rested.
I have been getting low AHI, typically below 1 and very low to near-zero leak rates. I mouth tape. I'm not sure if it is just because I'm averaging 6 or so hours a night that I feel so terrible in the morning or if it is my RERAs (UARS) causing it after the sleep apnea is under control.
What do you think of my chart for last night? It was almost 6.5 hours. I need to get that to 8. Working a lot lately and my body doesn't want to turn off early enough to go to bed at the time that I need to.
I switched it over to CPAP mode. I'm not too familiar with that mode. I still see "ramp" options available, but I have set it at 9 all night. I felt pretty decent tonight, so going to give that maybe 2-3 weeks to see how I do. Particularly on the weekend when I sleep more.
Does my breathing look okay or too shallow or anything? I switched to CPAP because I feel like the ramping up and down throughout the night might actually be waking me up from the pressure changes and I also feel like the CPAP being constant would hold my airway open all night long to help avoid the RERA's to begin with, since I understand them to be between a snore and an actual apnea. Is this a good idea?
I was originally 5.2 AHI and 18 RDI. UARS suspected.
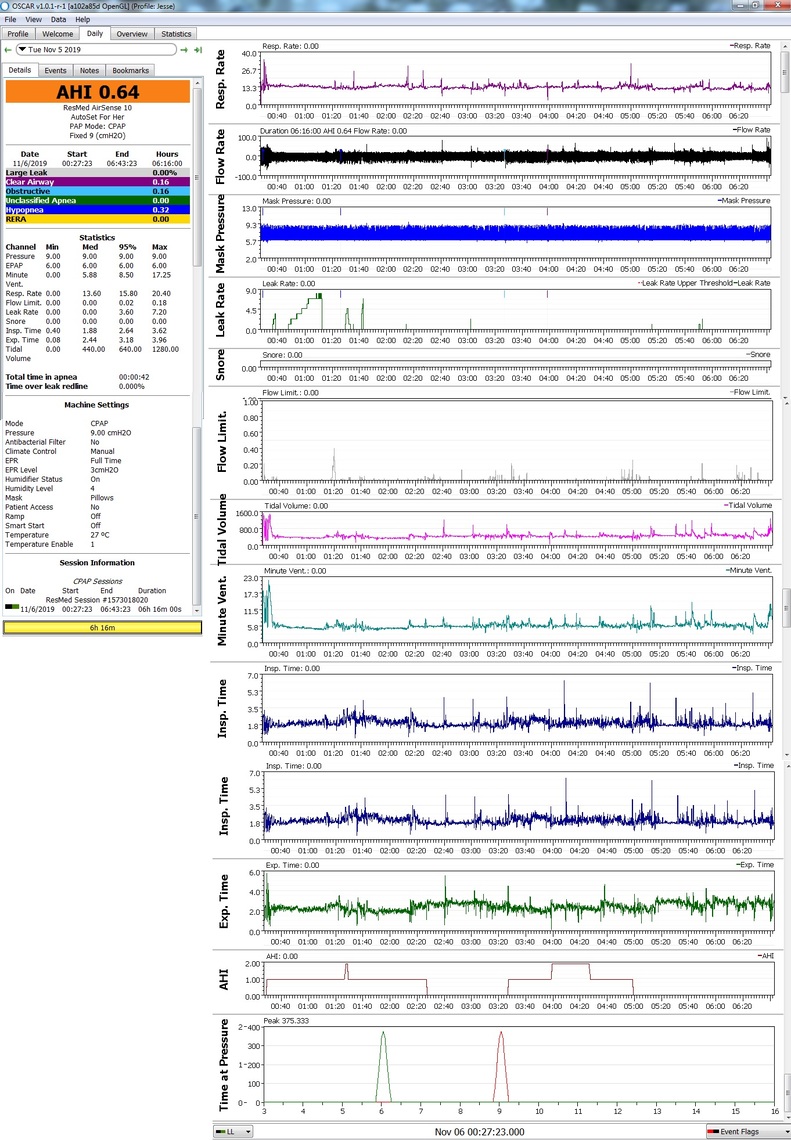
I think I'm going to have my thyroid re-checked again and get some blood work. My understanding is that it can cause breathing-related problems if it is not functioning properly. From last night, I see 4 central apneas within a 15-minute span. That started a few hours after I was asleep and just that cluster of 4 of them and then no more showed up. AHI of 0.66 on CPAP mode with 9 constant pressure and 6 EPAP. That seems to be my sweet spot for the numbers, I just still feel really horrible and I'm thinking there's something else going on. Could be just the pressure, though 9 isn't really that high of a pressure. I mouth tape and leak rate was 4L/Min. Obstructives are certainly under control. Unsure if there are non-visible RERAs still going on at this time. I do feel more energetic than usual, but still get hit with sleepy spells around 3pm to 5pm. Those look like genuine centrals where the breathing gets low very quickly and just stops for about 15 seconds before starting again.
I think your readings during the night look pretty normal. My recollection is that you have come a long way in getting a longer uninterrupted sleep. The recommended target for sleep is 7-8 hours at night, and ideally no naps during the day.
It looks like a constant pressure is working well for you. It looks like you are using full time EPR at 3 and no Auto Ramp. My suggestions for changes would be:
This way you will get 7 cm of pressure on inhale and 4 cm on exhale while going to sleep. Then when you go to sleep you will get a constant 9 cm on inhale and exhale. The problem with having the EPR on full time is that it reduces pressure down to 6 cm on each exhale, and you could be getting obstructive apneas at that point. In other words the effective CPAP pressure you are getting is only 6 cm. If you go to ramp only EPR your effective pressure is 9 cm. I think what you might find if you go to ramp only EPR you could reduce your CPAP fixed pressure from 9 cm to something lower, perhaps as low as 7 cm. That would likely make wearing it more comfortable, and it would also likely reduce the central apneas.
I see that SleepyHead is reporting that the climate control is in Manual. That may be a reporting problem. In any case I find having it in Auto is most comfortable if you have a heated hose.
That is about all I can suggest for improvements.
Climate Control shows as Auto on the machine. I've always kept it in Auto. Not sure why Oscar is making it show as Manual. I do have the ClimateLine hose and I keep it at 80F and preheat about 15 minutes before bed so that it is ready.
I used to like having the ramp feature on to start at say 6 or 7 and then ramp up to whatever was needed, but I felt like each ramp was waking me up and decided to try CPAP. I had camera footage of myself jolting awake in the middle of the night looking around to see where I was at. I feel like a constant pressure throughout the night helps me to sleep better and get less events than ramping up and down, for some reason. So now that I have the auto ramp off and it starts at and stays at the same pressure all night in CPAP mode, I have gotten quite used to this rather quickly. So instead, I start at 9cm and stay at it all night.
Should I simply play with the EPR and adjust it down to try to get used to it in CPAP mode? In the past even with Auto Ramp on, I switched EPR from 3 to 2 and I felt like I was suffocating.
I know that for normal nights when I'm well-rested, my required pressure with the ramp is 9. If I'm super tired, I'll have a bad night and it will ramp to 10 or 11 and cause centrals and a lot of events. 9 seemed to be the max number that I knew would clear my obstructives, but there was doubt on my behalf as to whether or not it was enough to prevent RERAs. Those central apneas look like I'm stopping breathing for 15-20 seconds on average. They were also rapid-fire in a row at only a certain time of sleep halfway through the morning. I wonder if I have a touch of central apnea that shows up during a certain stage of sleep? Neither sleep study detected it, however. I have also had a lot of nights where AHI was 0.5 or so and there were absolutely no centrals or hypopneas anywhere. Just like one apnea for the whole night.
My biggest concern was that my breathing seems to look quite shallow sometimes.
It looks like Oscar has some of the inaccurate setting issues that SleepyHead had. What your machine says is the accurate way it is.
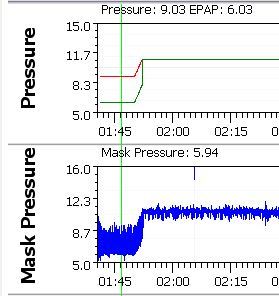
I think you may be confusing pressure ramping during the startup phase with during the night. You can still use AutoRamp when your machine is set into fixed pressure CPAP mode. That is how I have mine set. The AutoRamp ends when you go to sleep. It will not go into that mode again unless you get up and shut the machine off. If you do that, it will AutoRamp again until you go to sleep. This is what my machine looks like with AutoRamp turned on. I have mine set to an initial pressure of 9 cm, with a 3 cm EPR for Ramp Only. The pressure cycles from 9 cm down to 6 cm on each breath until I fall asleep. Then it ramp up to my fixed set pressure of 11 cm. This is what it looks like. The purpose is to make it more comfortable when you are going to sleep, and more effective when you are asleep. You are highly unlikely to have any apnea events while awake.
In addition to put the AutoRamp back on, I would suggest turning the EPR to ramp only, and making your fixed CPAP pressure 8 cm instead of 9 cm to see how that works. If your AHI is acceptable at 8 cm you may then want to move your fixed pressure down to 7 cm. It is kind of trial and error to see what the minimum pressure you can get away with is. With EPR off, you should be able to get effective treatment with a lower (more comfortable) pressure. Also, the lower your pressure the less likely you are to have central apnea events. Shallow breathing is usually what preceeds a central apnea event. If you use the arrow keys to zoom in on your breathing before a central apnea event you may see a shallower and shallower breath pattern, until the breathing stops and a central apnea occurs.
Hope that helps some,
Curiously, last night I tested the CPAP with the ramp still off, pressure at 9cm fixed and I lowered the EPR from 3 to 1. Breathing seemed more labored (I expected that and that probably would take a little while for the lungs to get used to pushing out air against more pressure) since it wasn't lowering as much upon exhale. However, I also wanted to see what it would do for how I felt the next day. I did feel more energetic today, but I also got a full 8 hours last night with the mask on, which is rare in itself and I'm still working on that. That's probably why. However, lots of events last night. 3 CA events and 6 obstructives. It felt like the EPR being set down was actually pushing the soft palate in my throat somehow and causing me to have more blockages, so that's kind of odd. Since I was a kid, I have always had this thing where I can blow air out of my nose and if I do it hard enough, it is like my soft palate blows up and causes a blockage of the air trying to escape from the throat to the sinuses. So that may just be something odd with my soft palate being a little larger or extended somehow. It puzzles me now why setting my EPR down lower actually causes more CA, obstructives and hypopneas.
I think the higher pressure must be causing CA events simply because more air is blowing to the point where the exhaled air with CO2 doesn't have as much of a chance to escape before being bumped out of the way with new air to inhale; so more CO2 is breathe in again than normal, potentially causing central apneas. At least, I speculate. Could be wrong.
I don't know why, but I actually have gotten so used to the pressure now that I feel good simply starting at full pressure and staying at it without using autoramp at all. My last "best" results so far on no ramp CPAP mode were at 9cm with EPR of 3. I had 1 obstructive, 2 centrals and one hypopnea for the whole night.
Every central event that I looked at, the breathing got slower and the chart measurement got lower until it virtually flatlined and then I started back breathing normally again and it went back up. In spite of the in-lab study (2.75 hours) and home sleep study (6 hours) saying that I didn't have central apnea, sometimes I think I might have just a touch of it on top of OSA. What I'm seeing on my nightly charts looks like legitimate CAs even down to the seconds where it just drops off and I stop breathing and start again. Yet there's only about 3 or 4 of them even on a bad night. I could lower the pressure from 9cm, but that's what is required to get my AHI down as long as it was between 0.5 and 1 on a typically decent night. Adjusting the pressure down to 8 would likely cause more OA events and maybe even centrals, so it is all a bit confusing and almost seems backwards in my case.
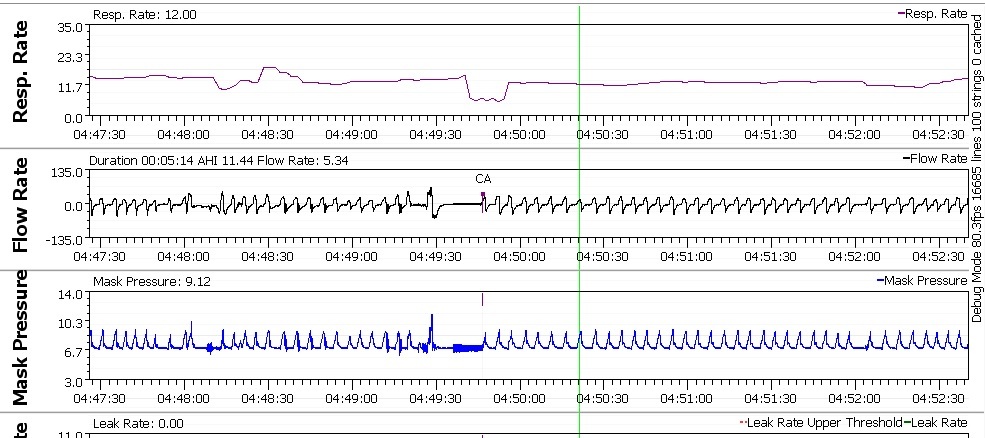
I'm attaching a quick grab of one of the CA events from last night. Definitely looks like a real central event to me. Also, before the one that was marked by the machine...I see one that wasn't marked by the machine and wasn't quite as pronounced, so it didn't label it CA.
So last night I tried 8CM pressure. Just to see, I didn't reduce the EPR and left it at 3. I would have expected my centrals to lessen. I had 4 obstructive, 3 hypopneas and 3 CA's. Less than the 3 CA events and 6 obstructives the night before. Should I try for 7cm pressure and probably take the EPR down to 2 or 1 or maybe even off completely? That makes me even more curious because I've lessened the pressure and had less obstructives last night. Normally, of of course...lessening the pressure would cause obstructions to increase because it isn't sufficient enough to keep the airway open. The only thing I can think of is that on exhale it might be messing with the soft palate in the back of my throat causing it to umbrella out on exhale.
I doubt that the EPR is doing you any favors. Think about it this way. If you set pressure is 8 and your EPR is 3, then you are getting 8 cm on inhale and 5 cm on exhale. You are most likely to have centrals on the inhale higher pressure and obstructive events at the lower 5 cm exhale. My suggestion would be to:
This will give you 7 cm on inhale and 4 cm on exhale while you are going to sleep. Should be quite comfortable. However, if you feel short of air, change the initial pressure to 8 cm. When you are asleep you will be at a constant 8 cm. This is lower than your 9 cm, and it is not being reduced on exhale, which should reduce obstructive events.
If this works you could then try 7 cm for CPAP. This will require the ramp start pressure to be reduced to 7 cm as well.
You really cannot compare one night to another. It takes a minimum of 1 week, and ideally 2 weeks at the same settings, so you can get an average result. Then compare it to the average result of another setting. You will end up chasing your tail, if you try to compare one single night to another.
Alright, so I did start pressure of 8 (didn't want to try the 7 yet) and EPR of 3cm on Ramp only.
2 hypopnea events and one obstructive for the whole night. I also had the craziest dream(s) this morning, which I think may be because of getting more REM-related sleep than normal. Some of them seemed like they lasted forever. Zero centrals showed up, so it probably is that EPR messing it up.
I saw a bit of odd looking, choppy-like breathing that I'll take a quick screenshot of later and post just because it looks so strange. Otherwise, I feel pretty good. I also went from medium to small on my Dreamwear nasal gel pillows. The Medium was more like a larger and the small is much more comfortable and doesn't cause painful sores on the bottom sides of my nose, so that is also helping. Just got that yesterday, as well.