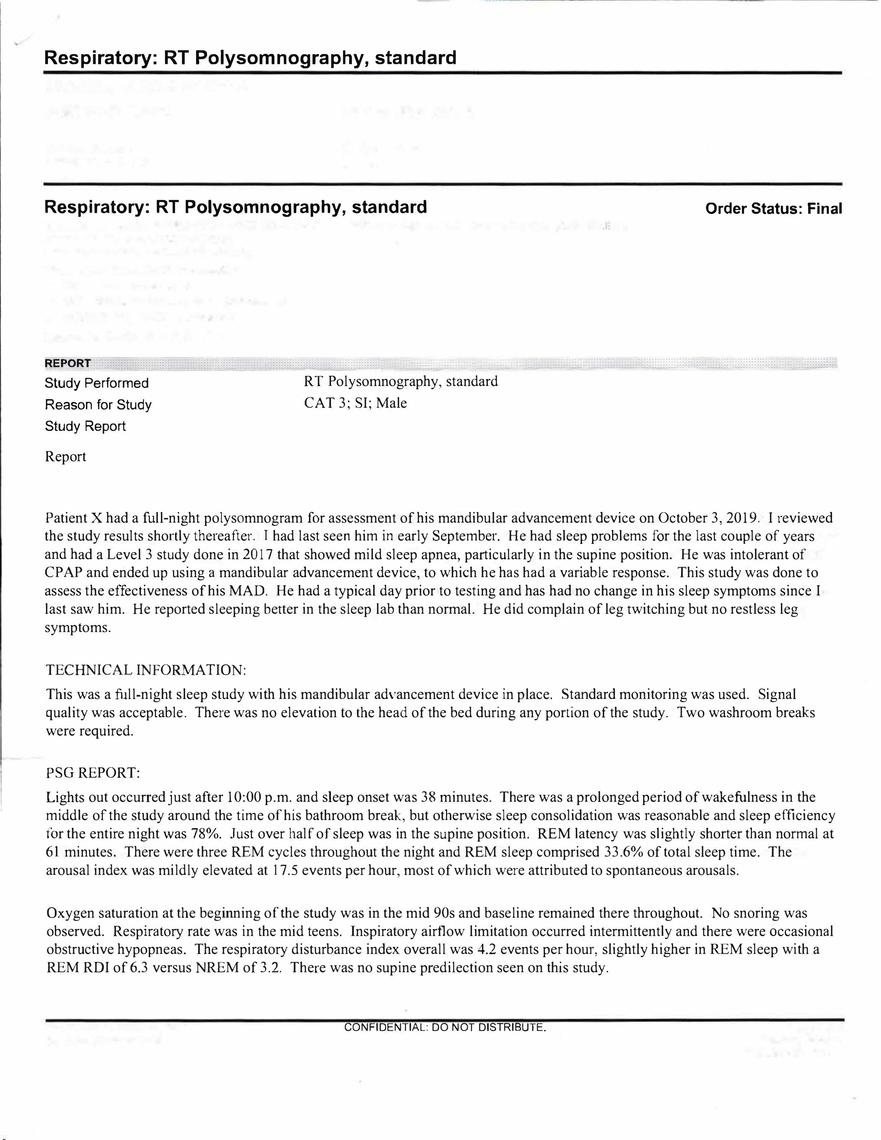
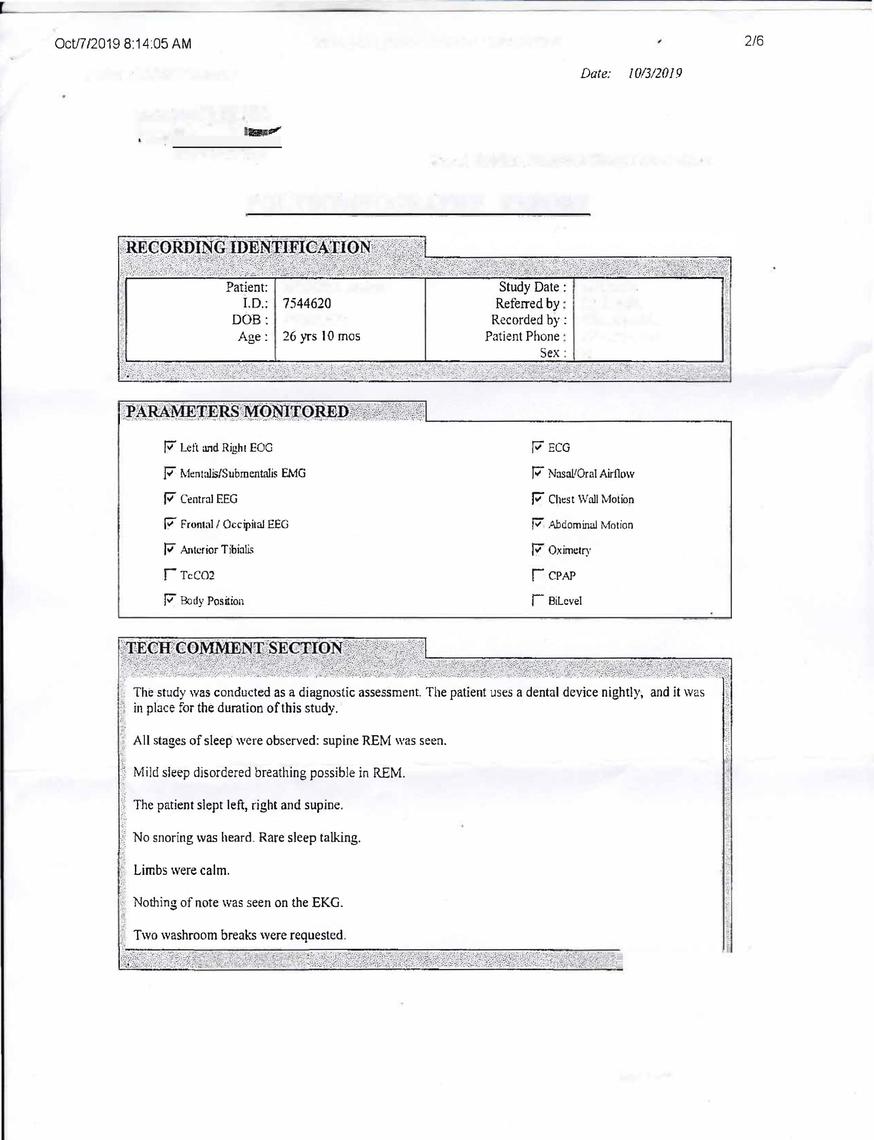
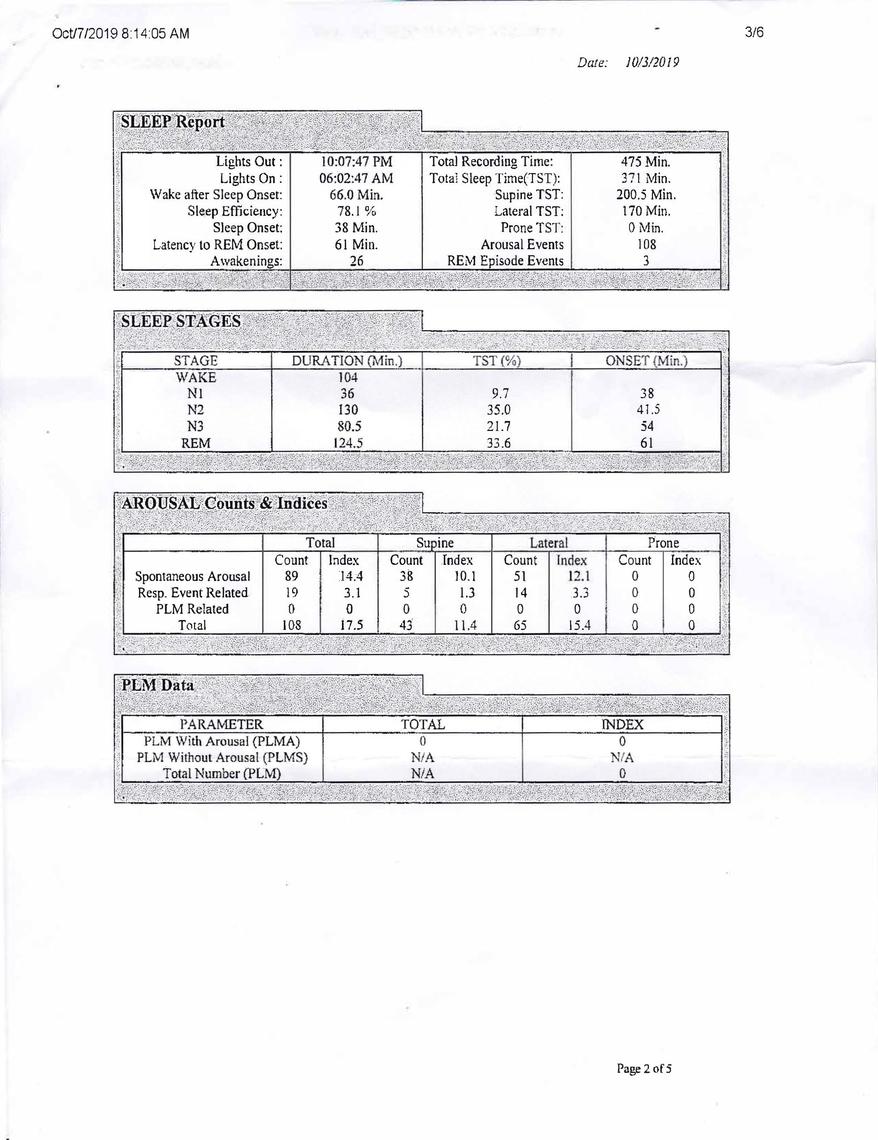
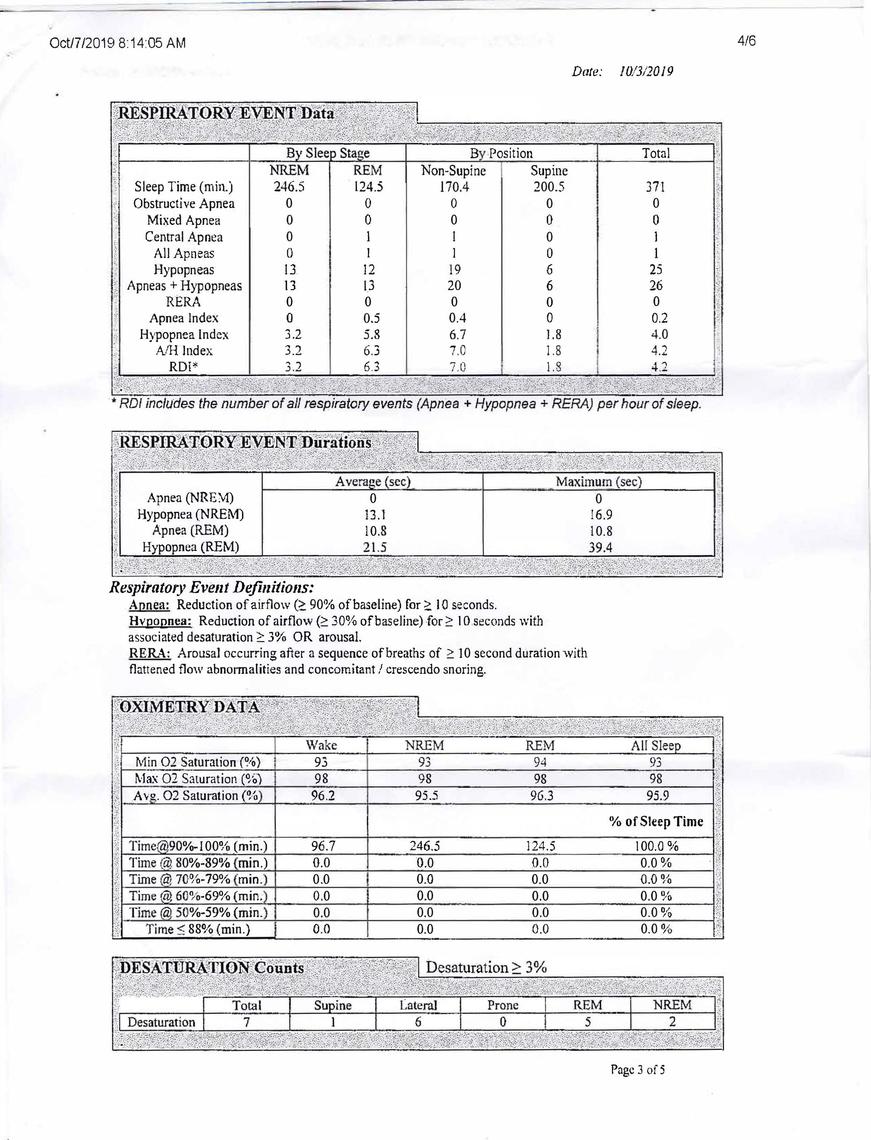
Hey Tjack. I'm a 27 year-old who was diagnosed with mild obstructive sleep apnea. A level-three study that included sleeping on my back showed an AHI of 7.8, and a level-one study that included me sleeping on my back showed an RDI of 4.2, but I wore a MAD. I'm healthy, skinny, and physically active.
I tried wearing CPAP for about three years, and I tinkered with settings (i.e. pressures, ramp, humidity, etc), masks (i.e. nasal vs full-face), my diet, my level/types of exercise, and overall sleep hygiene habits. I tried nasal dilators, CBD oil, sleeping pills, nasal steroids, and even lavender oil. I've also spent countless hours reading clinical literature, reading through sleep forums such as these, and even recording my own personal sleep data to analyse. Throughout the entire trial period of three years, I was still experiencing the same exact level of fatigue when wearing the CPAP by the end. I spoke with Ear-Nose-Throat doctors, respirologist sleep specialists, multiple general practitioners, and my family doctor. No one had any answers to the question of why do I feel fatigued (more tired than usual) when I wear the CPAP?
I hope I haven't pushed you to lose hope, but I just want to be open with you and perhaps help you avoid some of what I've gone through.
The first thing I would like to say is that there is data that indicates that it may take some time to "catch up on sleep" after experiencing untreated sleep apnea, and two weeks of CPAP isn't conclusive. Meaning, you may be playing catch up still, which explains your feelings of fatigue.
Second, when I spoke to my sleep specialist regarding the fatigue I feel after a night of wearing CPAP, he said to me that it's probably because the CPAP is doing more disturbing than helping, as I only have mild sleep apnea. I realize that is vague, but essentially he didn't have an answer (nor does anyone else insofar as I have looked), but he said that it is something he sees in patients from time to time.
Third, there is research demonstrating that CPAP for mild-sleep-apnea patients is often ineffective.
Now, with all that said, there are other options available, and there are small changes to lifestyle/sleep hygiene that can also go a long way in improving your quality of sleep/lowering your AHI/RDI. And, as mentioned before, you're too early on in the CPAP trial to come to any conclusions regarding your compatibility with CPAP as a treatment, so give it some more time and try working with your sleep therapist. The pressure just might be too high or you may be acclimating to the disturbances that CPAP engenders or nasal patency may be poor. There are so many angles to work from, and I'm assuming many of those are still unexplored by you. Sleep-apnea treatment is very individualized. There's no one-size-fits-all treatment plan out there, so start tinkering with the variables, and feel free to post here whenever you're dealing with unanswered questions.