Time for an Update...
CPAP THERAPY
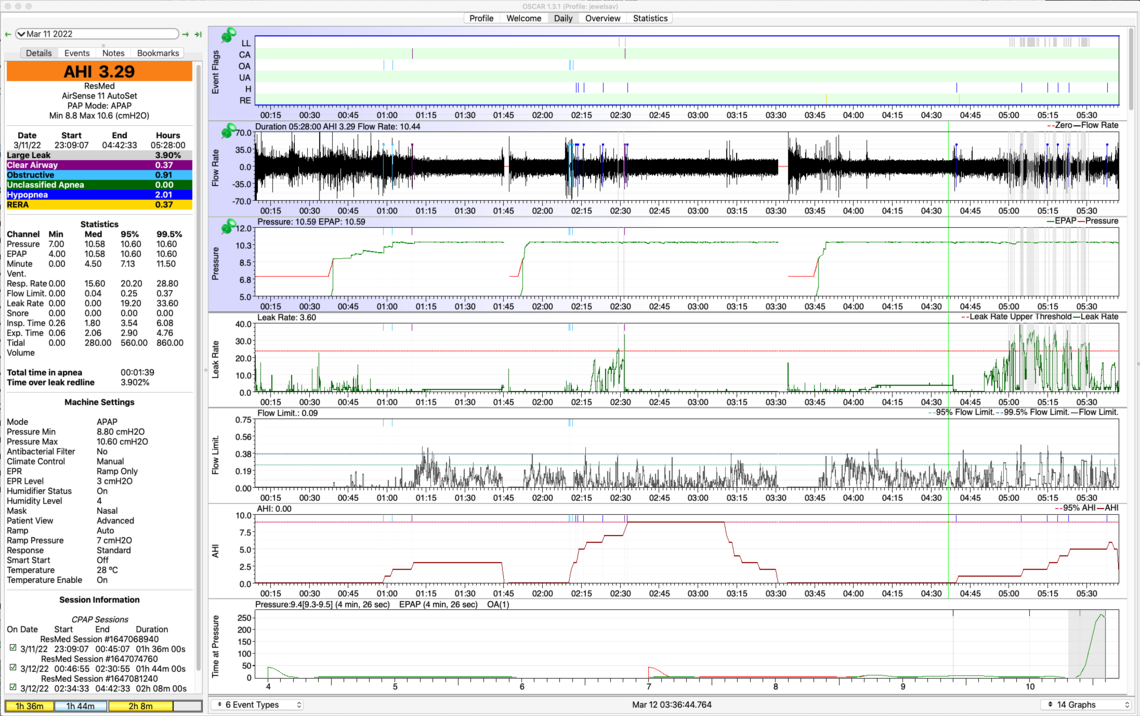
As you suggested @Sierra, I made a change on Mar 17 from Min/Max 8.8/10.6, EPR: Ramp to Fixed Pressure 10.4, EPR 1. After 1 week, AHI, OA, H and R are all down significantly. Yippee!! But CAs are up slightly. So, for the next week, I will try lowering the fixed pressure to 10.2, while maintaining EPR=1. See https://docs.google.com/spreadsheets/d/122kA5EJiwUXKilxmQYR6FRRvGxNRau7Tufwssk3-Etw/edit#gid=0 for details.
AHI down from 5.16 to 2.50
OA down from .48 to .37
H down from 2.14 to .77
R down from 1.91 to .53
CA up from .63 to .87
SLEEP QUALITY
Fortunately, my jumping out of bed like a ninja, and screaming like i'm in a horror movie have ceased. My parasomnia diminished to speaking in a conversational tone, my not waking up, and having no recollection of dreams (my husband reported the events). Then, at least for a week, all these events have disappearing altogether. We purchased a Wyze outdoor camera for ~ $35, mounted it with a wide angle view, so for the next few weeks I can see if I have sudden movements or outcries. I expect these behaviors/vocalizations may appear from time to time, but this is a vast improvement over events happening 2-3x/week. I had a preliminary diagnosis of RBD, but it (hopefully) will turn out to be pseudo-RBD with parasomnias brought on by sleep apnea and long term sleep deprivation.
I still wake up 2-3x/night, and get only 5-6 hours of sleep/night. I am waking up a tiny bit more refreshed. From reading others' experiences on this forum, I figure it may take weeks to months to feel less tired. Any suggestions are welcome.
DEALING WITH $#@&
My (excellent) sleep doctor referred me to a movement disorder neurologist within the same health organization (Stanford) to run some tests to determine if I have RBD. It took 3 weeks for the Stanford neurology department to decline the referral and tell me to contact them again in December 2022, at which time they "may or may not" schedule an appointment for me sometime in 2023. I emailed my sleep doctor and asked for a referral to UCSF (US News & World Reports rates the UCSF Neurology department #1 in the US). My dr's admin assistant (without even showing him my request) emailed me back that Stanford has a policy of not referring patients outside their system. Fortunately I had a zoom call with my dr yesterday. He was dismayed that there's such a policy (if there even is one, since he's never heard of it), and said simply "Why would I do that?"
Between the time I heard back from the ding-a-ling assistant until I saw the dr, I asked my primary care physician to make the referral, which she did within 24 hrs. As it turns out, my sleep dr and the UCSF neurologist are good friends and did their sleep fellowship together. My dr highly recommends the neurologist. He offered to pick up the phone and call her then and there to make the referral, if I wished. He lamented, "We both work for organizations with a lot of bureaucracy."
So while I feel I am in good hands both with the sleep dr (who gave me his direct email for future communication) and the neurologist, roadblocks and obstacles continue to suck the energy out of me on my journey to get a good night's sleep.
Another energy-drain is the DME. I have asked for six weeks for nasal cushion replacements for my Airfit N30i mask, which should be replaced every 2 weeks. I finally raised my voice, and was told they weren't in stock, the DME would have to order them (wouldn't give me a time estimate), and then they would have to go through the usual shipping channels (+1-2 weeks). Then I raised my voice even louder, screamed a bit, and lo and behold, the nasal cushion replacements arrived 3 days later. With the old cushion, I was experiencing a sore throat and headaches. I used a new cushion last night - woke up just fine.
Thanks for allowing me this one-time rant. I realize everyone on this forum has stories like these and worse. Why does it have to be this way? Sigh. I'm just so awfully tired of these nuisance roadblocks. This has already been a 3-yr journey to get to this point - I won't bore you with the details. But now I have the finish line in sight, thanks in part to the help you have generously and compassionately given me. I am truly grateful.