Hello,
How effective CPAP is at treating central apnea?
My understanding is: obstructive apnea is when tongue or other soft tissues in the throat prevent air from flowing. Central apnea is when act of breathing is not happening.
For obstructive cases CPAP applies pressure from outside and it stops tissues from collapsing - breathing happens.
How does it help for central apnea?
If you have a bilevel machine designed to treat Central Apnea it works quite well. Obstructive Apnea is treated with Exhale Pressure (EPAP) on bilevel or pressure on CPAP. Hypopneas and Flow Limitations are treated with Pressure Support (PS) on bilevel or raising pressure on CPAP possibly utilizing EPR to mimic Pressure Support. CPAP and BiLevel without backup are not intended to treat Central Apnea, when Central Apnea is present on these machines is by avoiding the Central Apnea (lowering pressure and/or EPR). A BiLevel with backup treats Central Apnea either with full time Backup, which means on a timed basis increasing the inhale pressure significantly over exhale pressure by enough to force an inhaled breath, then dropping off to allow an exhale. An ASV (adaptive servo-ventilation) is designed to keep pressures as low as reasonable, applying the higher pressures only during a Central Apnea event.
That is not enough info to advise you other than to say it needs to be looked at. I would like to see a redacted copy of your full sleep study. I'm interested is any mention of Central/Mixed/Complex/Treatment-Emergent Apnea in your diagnostic study. It is frequently left out of the summaries. If there was no mention it is likely that this Central Apnea will go away in 2-3 months.
To get a better idea Post SleepyHead data with the following
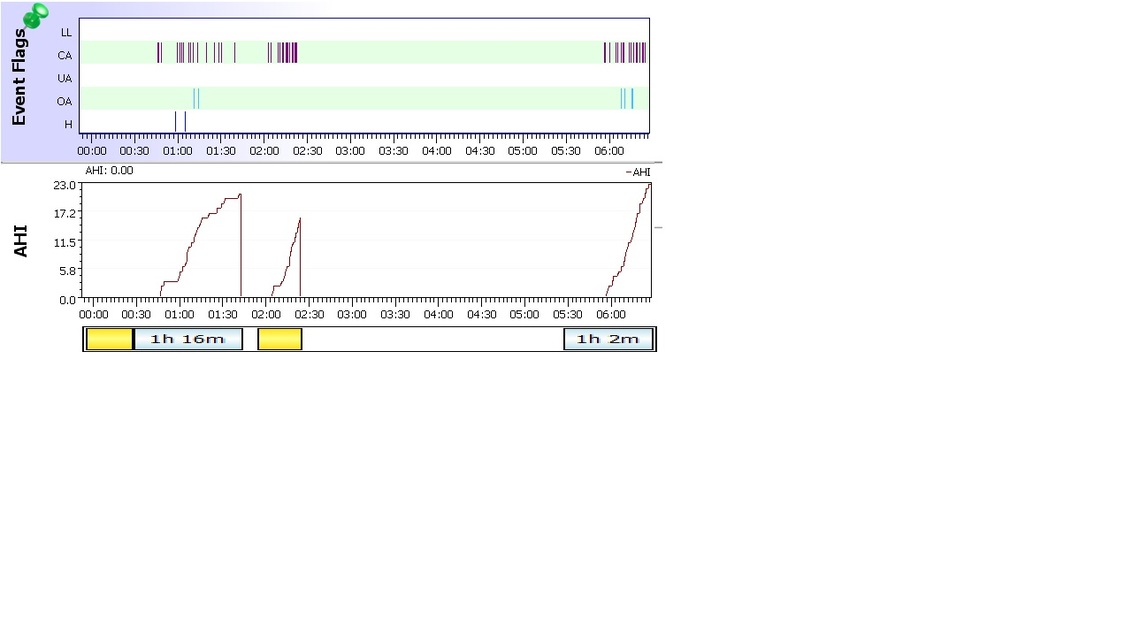
The most useful charts for diagnostic purposes are:
Event Flags Flow Rate Pressure Leak Rate Snore Flow Limit (Resmed Only. Respironics includes Flow Limitation in Events) Each chart has a name displayed on it vertically on the left side of the chart.
You can move a chart up or down in the order by pointing your mouse pointer in the label part of the chart, left clicking and dragging up or down to change the order.
The chart height can be resized by pointing your mouse at the border of a graph until the cursor changes to a double bar with an arrow above and below, then dragging the border up or down
Also include the left sidebar so we can see important stats and your settings. Please remove the PieChart and Calendar.
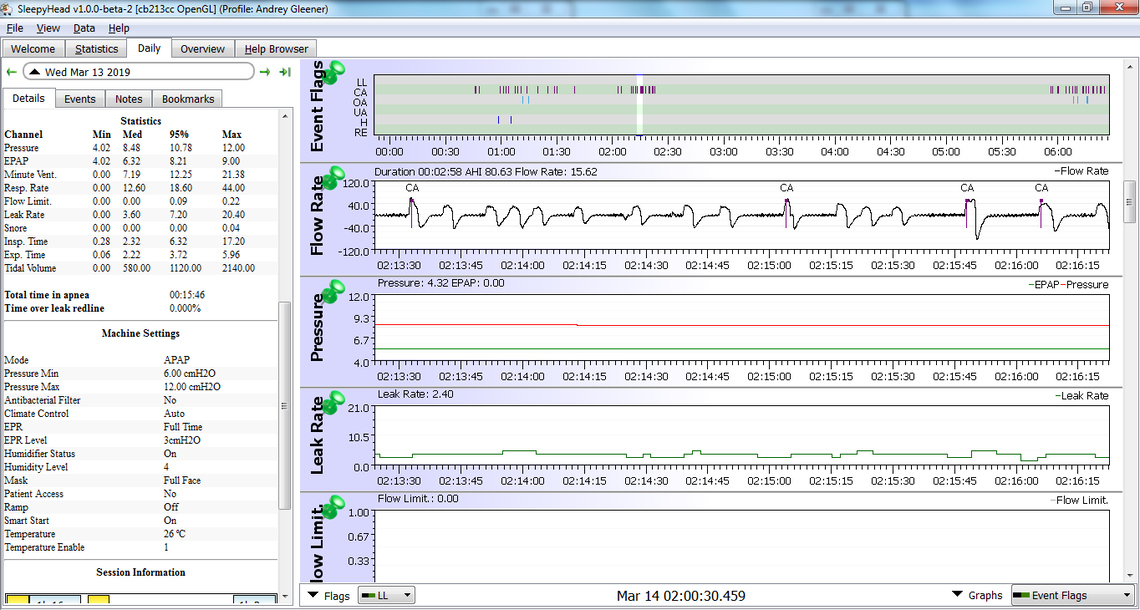
A second chart, same info but zoomed to show a 2-minute Window (left click) showing the CA events near 2:15AM so we can see the wave form in the Flow Rate
That should provide the info needed to best advise you of what is going on.
Andrey, IMHO those are legitimate Centrals assuming that you were asleep. You, in this segment, are having many events that are too short (<10 seconds) to call. Missing are the colored bars right above the statistics in the left sidebar. They tell us the breakdown of your AHI. FYI Snore, Flow Limitations, and Events are important because they are what triggers pressure rise on your APAP.
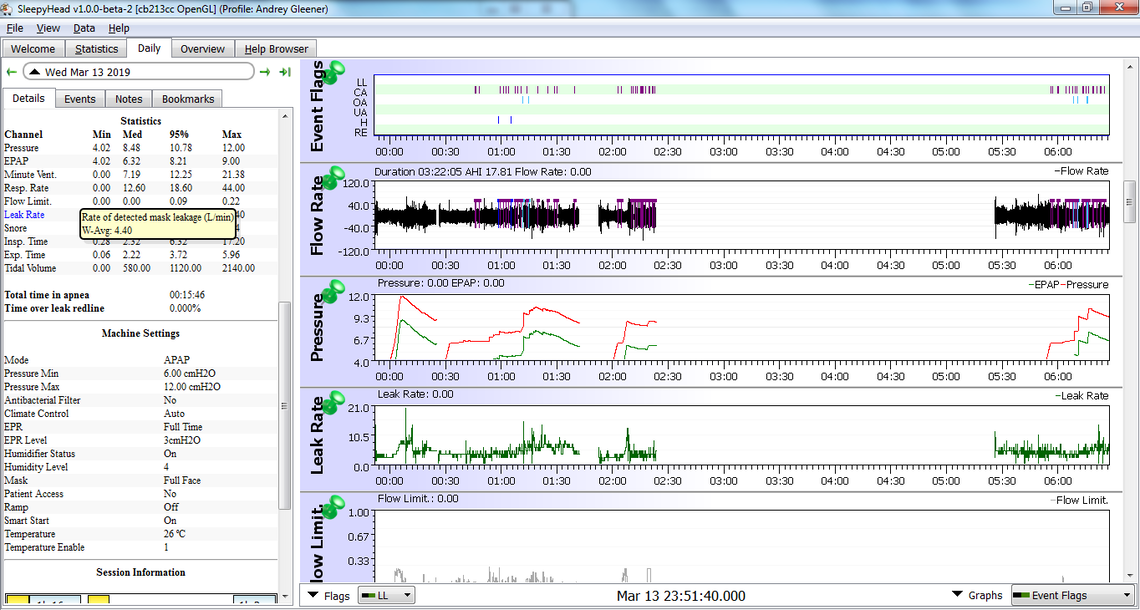
I'm going to suggest that first we decrease your EPR to either 1 or off. This is because the pressure variance from EPR may be the cause of your Central Apneas. then post again with charts. (Only 1 change at a time, that way you know what caused the response. Another change I'm anticipating to lower your max pressure.)
Do you have a Pulse Oximeter? If so post the results. I would expect to see a few desats based on the grouping of your Central events. On the next set squeeze the Flow Limit, Leak Rate, Snore for the main chart and add Minute Vent, Tidal Volume, and respiration rate to the expanded view of some CA events. I would unpin everything but events and flow rate. You can change the order by grabbing the graphs and moving them adding Minute Vent, Tidal Volume, and respiration rate below the standard then you can just scroll up.
Another item of note is your max Respiration rate of 44. That is essentially panting. I'm not overly concerned but I'm sure that caused an arousal.
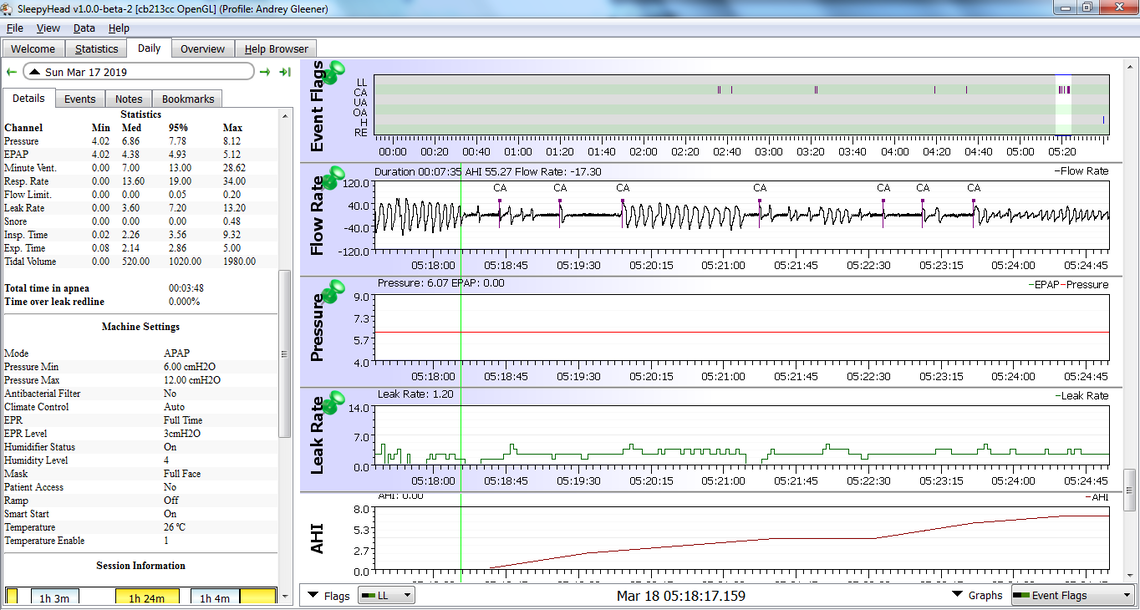
last night was pretty bad again. So bad that I am lucky to be alive now. There were sequence of events when i could not breeze up to 30 sec. It is now an emergency and i do not know my actions. What steps i should take to stabilize situation? the girl who runs CPAP shop is of not much help. See attached snippet
I'm going to suggest that first we decrease your EPR to either 1 or off. This is because the pressure variance from EPR may be the cause of your Central Apneas. then post again with charts. (Only 1 change at a time, that way you know what caused the response. Another change I'm anticipating to lower your max pressure.)
I have central apnea as well and I am being Treated at BI in Boston. They are using a novel treatment with a regular cpap instrument. It involves modifying the mask so it’s not vented and including a length of vent hose as a co2 trap. The objective is to slightly increase the rebreathing of co2 to trigger the resipitiry response. I find it extremely effective. I would not try to do this your self but it may be worth looking into.
[http://www.apneaboard.com/wiki/index.php?title=Enhanced_Expiratory_Rebreathing_Space_(EERS)] Enhanced Expiratory Rebreathing Space (EERS) This is an option for the treatment of therapy onset Central Apnea with CPAP This is a much less expensive option than getting an ASV machine. EERS is discussed in this wiki with contact information to the doctor and DME researching this option. EERS works by maintaining enough carbon dioxide in the breathing circuit to prevent central apnea. Please feel free to show your doctor this information and request that he consult with Dr. RJThomas, or prescribe an EERS mask from the DME.
The trouble with this therapy is finding a doctor or medical facility which utilizes this treatment.