Thank you for the help. I will let go for now of my recent obsession with events flagged during Large Leaks. What I consider bizarre is how during LL sessions 70 OA events can register over 30 minutes. That is suffocation, and I don't think it is accurate.
If my machine is set to past 10 cm pressure no full face mask will stay sealed on me. I call it a blowout when a seal cannot be made. By week two on a new mask cushion, I have to cinch straps tighter and tighter to keep leaks down. It becomes painful.
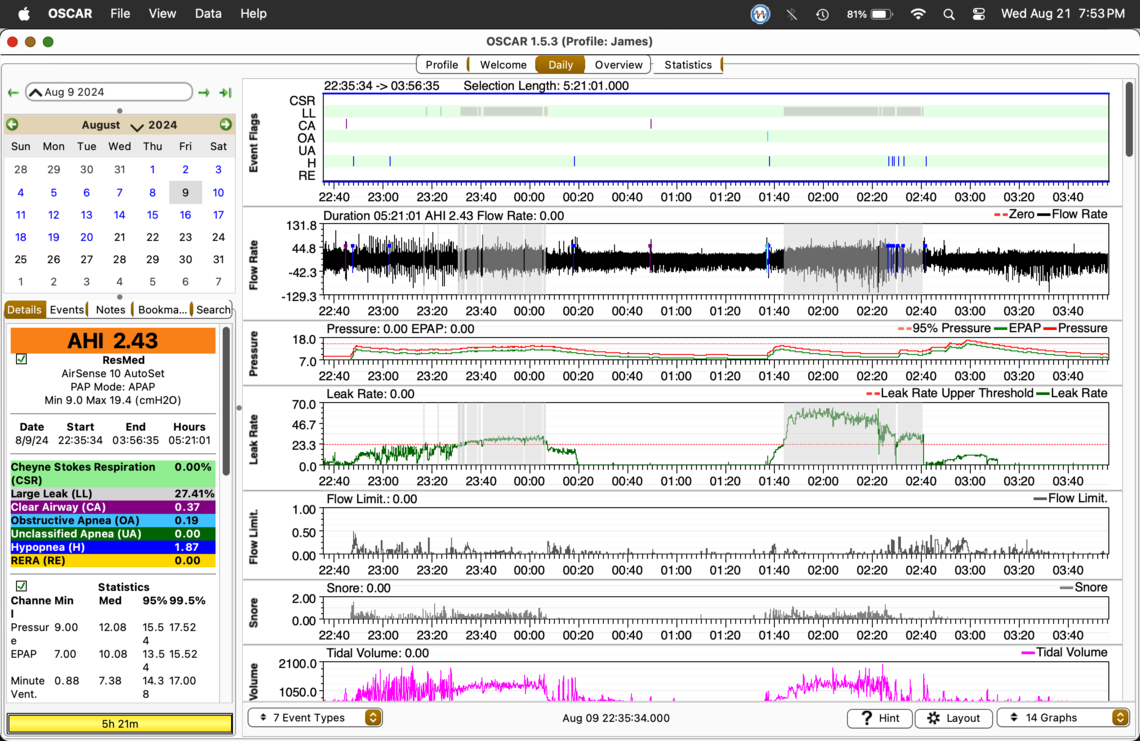
Using APAP I have recurring themes of pressure up leaks up and leaks up pressure up. I tried straight CPAP @ 8 cm and had the worst AHI ever... 17.00 so back to APAP.
I raised my Min. pressure to 9.4 cm using my new F40 mask. Flow limitations went down but the rise in CAs caused an unusually high AHI yet I think therapy went better than usual. Two rested days in a row with my new F40 mask is very impressive. Leaks went up, AHI went up, but I felt more rested than I have in years. Finally, maybe a mask that somewhat works.
CPAP therapy has been very disappointing for me for over 17 years. I see a doctor once a year. Nothing is checked or disgusted. It was just last year my compliance was verified. For 14 years I complied with therapy even though it never made me feel any better. I am sure I am not alone. With time to get into the nit and grit of OSCAR reports over the past couple of years, I just may be on the verge of effective therapy. If it were not for online volunteers like you I would have no guidance...AT ALL.
Maybe someday CPAP machines and OSCAR will be at a higher AI level and be able to fine-tune therapy on the fly.
My next quest is to copy/paste my OSCAR Statistics to a spreadsheet and then produce line graphs from the data. The bar graphs of OSCAR Overview are too busy for me to track trends. It is a sort of "can't see the forest for the trees," effect I get from staring at those bar graphs.
Best of luck to you and your wife. ejb