I’m a 44 yo male, a masters athlete/swimmer, 24.1 BMI, on 12.5 hctz for bp control (120/70 avg now) and just began taking a low dose of levothyroxine to treat a mildly high tsh (4.1). Back in September I began feeling fatigued, unable to concentrate at work and sometimes feeling a bit loopy or lightheaded. My md asked about my sleep but I was sure I didn’t have a problem there and wanted bloodwork done to check for anemia or vitamin deficiency. Nothing was really abnormal other than vitamin d in the upper 20’s and in December for a routine checkup my tsh had risen again to over 4 which has happened a few times in the past 4-5 years. Finally agreed to a home sleep study. Results as follows:
Ahi 3 Oai .6 Cai .4 Hyp index 1.8 Odi 2.6 Avg sat 95 Lowest desat 90 Lowest sat 82 Min pulse 45 Max pulse 136 Avg 58
4 osa 3 csa 13 hypop 113 snore
I know that I can slide my jaw back and more or less cut off my airway when I’m awake. I’m assuming this occurs when I sleep so I’ve been trying to sleep on my side or stomach. I do wake often at night. Sometimes with no consequence and I fall back asleep quickly. Other times I feel anxious with a heartbeat that isn’t high but feels strong and keeps me awake for hours. I do have an appointment with a sleep doctor but it’s not for another month so I’m looking for some insight. What might I be looking at for treatment? The centrals scare me a bit. Is that fear justified? Are these numbers enough to cause a person to feel fatigued and such? I’ll add that I do have days that are better than others. If I sleep well, most often on weekends, I have pretty good days. I almost thought I was through the woods this past weekend but then Sunday night I lost 2-3 hours of sleep tossing and turning.
Apologies for the long winded first post. Any assistance or advice is greatly appreciated!
-Matt
I am not a medical professional, but from what I know about apnea, your readings are in the normal range except for the moderate desat numbers. Did your study make any note of RERA (respiratory event related arousal) events?
No mention of rera in the report. Thanks for commenting.
Not sure if it matters but this was a home study over two nights. My first night I slept terribly. Maybe 2-3 hours and then awake for another 3 or so. They had me keep it and try again which yielded a 5-6 hour sleep window.
Yes, if it was a home study, they typically do not flag RERA events. Most insurance companies will not approve a CPAP based on the RDI index which includes RERA events as well as apnea and hypopnea events. There is some controversy in the industry on how serious RERA events are. My thoughts are that if they lead to arousal, they certainly do not contribute to a good sleep. I would also expect that a CPAP would help reduce the incidence. That said, I still get 1 or 2 RERA events every night at 11 cm of pressure...
See this link if you want to take a deeper dive into RERA.
I checked out the RERA information and it sounds like what might be getting me. As an in lab study will be all out of pocket for me right now ($4500) my doc suggested just trying an APAP for a month. My concern is that I’ve read some comments here indicating that an APAP can make centrals worse, and I had 3 of them per my sleep study. Should I be concerned about this or just assume the doc knows what’s right?
Any suggestions on which machine? Resmed or Phillips?
I think if there is some economic way to try an APAP that is much more informative than an expensive sleep study. Yes, pressure can make centrals worse. The basic idea is to use the lowest pressure possible to treat the obstructive apnea and RERA without causing an increase in central events.
The issue is whether or not PAP treatment will be worth it for you. Have a look at other threads in this forum from those who have RERA and marginal apenea. Some success with PAP and others do not. There is a certain amount of discomfort with using a PAP machine, and the benefits have to offset that discomfort to make the net result positive.
On machines I am bias. I think the best APAP on the market is the ResMed AirSense 10 AutoSet For Her (even for males). It has an optional algorithm that can work well for those suffering from RERA and on the margin. It can also be changed into the regular program mode, and does not cost any more than the standard AutoSet.
If at all possible try to get into an arrangement where you can just do a trial with the machine, and also have the ability to try different masks. The mask is the often the most difficult part to get right.
So far I’ve had no luck with finding anything truly economical and am thinking I might just have to buy a new one and if it’s not the treatment I need or it doesn’t work out, just sell it, likely for a fraction of what I paid.
Thanks for the input on machines. I’ll keep that in mind.
I do have an appointment with a sleep apnea dentist in two weeks so will be curious to see what he suggests. I think the appliances are between 1-2k from what I’ve read but it seems they would be less frustrating to use than a pap machine. Of course, if you spend the money and it doesn’t solve your problem, then what?!
A concept that my feeble brain has been struggling with for a while is how you would use a CPAP machine to replicate a sleep study.
I can see how it could be used to fine tune parameters and settings for a CPAP machine but what else can it do beyond or before that?
I always think of a sleep study as gathering data without treatment or pressure. Trying to assess the extent of the problem before considering therapy.
I would like to know what my OSA and oxygen numbers are now without CPAP and can't afford a sleep study so if a CPAP machine really can do that I'd love to know about it.
I don’t understand why sleep studies cost what they do. My sleep doctor shared my sentiments which surprised me. Even a home sleep study through our local hospital is $1200. That’s absurd.
A home sleep study would only cost $100 out of pocket here.
Our national health scheme (Medicare) pays the rest.
But even so it's not easy money to find.
Home sleep studies appear to be moving towards mainstream medicine now but when it comes to skilled service nothing seems to have changed.
The person I spoke to today at a sleep study facility apparently had no specific training and admitted to having no knowledge of what the equipment monitored.
I'll point out that while it is not uncommon, most Apnea patients do not have a problem with Centrals, Sierra is one of those uncommon patients. I recently had Centrals to a level of .14 AHI. I ignored it. That will in no way influence me in my settings. When reviewing others data I always observe the Centrals, and address them when they need to be addressed. I look to see how they respond to pressure and pressure variance. The settings I suggest tend to probe to see how your body reacts and ultimately look for the settings that minimizes your apnea and provides you good comfort.
No attempt at auto CPAP yet.
So I wound up having an in lab Test. Slept pretty poorly as I rarely sleep on my back at home now with a fanny pack and tennis balls to hel/remind me, and also took a Benadryl to make sure I would sleep (sleep tech approved this).
18 central, 28 hypops for an ahi of 8.
No RERA. Longest Apneic event 17.2, mean 13.1.
Longest hypopneic 76 seconds mean 30.
Minimum O2 of 91%.
EEG normal.
Intermittent sinus bradycardia and sinus tachycardia. I’ve had some palpitations recently and switched to a new bp drug. Valsartan from hctz.
Sleep efficiency at 73 percent. 47 awakening, 194 stage shifts and 1 rem sleep period.
Most centrals on back. 14. 1 on left and 3 on right.
Most hypopneas on back. 20 back, 7 left and 1 right.
Any thoughts? I’m troubled by the centrals. Wondering where this came from all of the sudden...seemingly.
Also, the report suggested I do another study, titration for CPAP or BiPap. Naturally they would suggest this, at $6500 per study. I think I’ll have met my out of pocket max so the money isn’t a big issue now I suppose. Truthfully it’s not a great experience anyway. Very clinical, uncomfortable to sleep connected to all of the wires, etc. Can I push for an auto BiPap? Would that be out of the realm of reasonable, assuming I’m going to be using a machine?
Thanks!
CPAP's really only correct obstructive apnea, and it appears you have none. You are having more hypopnea than central apneas, but in the absence of any obstructive apnea or RERA, there is some possibility those hypopnea events are central in nature. In other words they are not a result of flow restriction, but the result of effort to breath restriction.
BiPap is not an obvious solution either. They (and APAP as well) use pressure to support the airway, and the pressure can have a side effect of increasing central apnea. Some BiPAP machine have a backup respiration rate. They cycle inhale and exhale pressure to give some forced ventilation, and can help with central apnea to some degree. The machine that is best designed to address central apnea is the ASV type. In the ResMed line the AirCurve 10 ASV is an example. The unfortunate part is that they are expensive. In Canada they run a little over $4000 the last time I checked. You also need a heart function test before they will be prescribed.
My thoughts would be to try and get an independent opinion from a sleep doctor that ideally is not in the business of selling sleep tests or machines.
Those are just my thoughts based on having significant issues with central apnea. Last night I has an AHI of 4.5 and it was nearly all central while using an APAP. I am not a medical professional though, and this is just an amateur opinion.
The other thought is that you could consider getting an opinion from a cardio vascular doctor. Central apnea can have origins in the heart and lung system.
I appreciate the feedback. With respect to machines, I wonder why they suggested CPAP or BiPap? Seems strange. The machine you suggested is about 3500 here. Wouldn’t want to be replacing that too often!
Looking at it a different way, it seems if I could totally eliminate the supine position from my sleep I’d have a very normal ahi. Maybe that’s the first step to take?
I think I’ll talk to my gp this next week and see if he might send me to a cardiologist. Honestly, not knowing where this is coming from is what scares me the most. Well, that and allowing this apnea to terminate my existence while I’m waiting on a diagnosis and treatment from my medical team. And having to wait weeks to discuss with your sleep doc isn’t good for impatient people like myself!
Obstructive apnea is certainly increased by sleeping on your back. Essentially it is a gravity thing with your tongue. It falls back and blocks the airway. Not sure how one could connect central apnea to sleep position though. It happens when the body does not attempt to breath. It is most often caused by the body thinking O2 is good, when it in fact is not, and then when it is too low, the body reacts too late. It essentially is an unstable control system, kind of like a cruise control that keeps chasing the speed up and down without getting it stable.
It’s not entirely logical to me either. I’ve had some abdominal and rib soreness off and on the past few weeks and I thought for sure it was related to OSA. You know, struggling to breath against the resistance of a restricted airway. But if it’s all CSA as this sleep study says then I don’t know. Also a bit odd to go from 4 obstructive and 3 central apnea’s on home study and now having all central apnea’s. To me anyway. I’m sure I’ll spend some time googling this over the weekend and maybe come up with some plausible explanations for some of this.
I didn't respond to your question about why they suggested CPAP or BiPap. I can't explain why they would suggest a CPAP. In the industry a BiPap seems to be always considered to be the next step if a CPAP doesn't work, although I recall one study that found in 60% of the cases a BiPAP provided no improvement over a CPAP.
Sierra has this nailed. The typical path to an ASV is to fail CPAP, Fail BiLevel without backup, Fail BiLevel with Backup, and finally succeed with an ASV. Fail means to fail to adequately treat your apnea.
Based on your in lab sleep test the best machine, IMHO the only CPAP variant that would be able to treat you is the ASV. But, you are currently mild enough that with good position management, sleeping on your side, and I do not understand why that would work for central apnea, should be able to manage your apnea. I ask how you could best monitor your apnea going forward to determine if it is getting worse.
On why the difference between the in lab test and the at home test. Were you in a strange bed, in a strange room, with a strange pillow? Were you fully wired up and had freedom of movement, were various contraptions connected to various parts of your body? The answer is obvious. While there is currently no better standard for determining SleepApnea than an in lab sleep test, it is just not normal, and those differences can account for the differences. The in Lab test had the electrodes attached professionally, these are a major indicator in determining Central Apnea so if your in home test was performed by a lesser qualified individual, with a different quality setup, the results, while similar, could easily be different.
Might I have messed up the sleep study with the Benadryl tab? It was only half a dose and the tech approved. I do sometimes take a Benadryl or a half dose of NyQuil on nights where I’ve woken up around midnight and been unable to sleep.
The bed was quite uncomfortable as were the pillows. But that’s all obvious I guess. I often sleep prone at least part of the night and was unable to do that. Oddly enough though, I felt slightly better than usual the day after. Of course I slept from 9:30pm to 5:30am and then went home and slept another 2-3 hours, so I got an extra 2 hours of sleep compared to my usual routine.
The fanny pack and tennis ball don’t always work as I sometimes find myself at least partially supine. Maybe I should get a more functional device that is meant for this purpose.
Your question about how to monitor going forward is a great one. I suppose it could be partially based upon how I feel. Or maybe an o2 sat meter that records?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2670330/
Has anyone heard of this before? Rather old I suppose but interesting nonetheless.
I believe that drug is Ambien, and I would be careful about getting into sleeping pills. Don't see how they would help centrals, but who knows... I believe acetazolamide is a diuretic, and I would suggest a little less of a risk. It is still off label to use for central apnea though.
Good point. Not too excited about getting into more medications if not needed, now that I think about it.
Looking at a few things other than AHI in my report and I see a few things that didn’t originally jump out.
14 arousals associated with respiratory events for rai of 2.4.
109 spontaneous arousals for index of 18.9. That seems terrible!
47 awakenings, 194 sleep stage shifts and 1 rem period.
Sleep efficiently at 72.9
It also says in comment section that the psg was notable for abnormal sleep architecture and sleep fragmentation as well as hypoxemia due to osa syndrome. But I didn’t have any obstructive events! Are the Hypopneas obstructive and resulting in central apnea’s?
So it seems like my spontaneous arousals and multitude of sleep stage shifts might be as damaging to my energy levels as the ahi number itself. Or am I off base?
Edited to say, I guess I did mention some of these things though they didn’t really hit me until I took another peek this afternoon.
You are traveling into difficult territory. I would think if the sleep clinic is credible they should help you with the interpretation of the results. For example, there is something that us amateurs call "sleep wake junk". It occurs when you semi awake and fall back asleep again. It can result in apnea events which some would call false. I think to some degree those that interpret the sleep study should identify this stuff. They have electrodes which should indicate the stage of sleep you are in. They also can correlate oxygen desaturation to the potential apnea events.
On the hypopnea you need to see the up close detailed flow data to see if the event is obstructive or potentially central.
About all I can suggest is getting a hard copy of the test results and getting a second export opinion on what it means.
So I finally had my appointment with the sleep doc. It was a bit rushed an not as informative as I’d have liked.
Anyway, he basically wanted me to get another sleep study/titration. Didn’t have a firm opinion on positional therapy other than just leaving that up to me. This seemed odd to me as my ahi supine is 13, left side 4.1 and right side 3.4. That’s a pretty significant difference to me. He did suggest that the centrals might not all be centrals as they could be obstructive that the respiratory effort just wasn’t significant enough to be caught. And of course, some centrals could be sleep transition related.
At this point I think I’m going to try a positional belt for a few weeks and see how I feel. If it’s not an improvement I’ll get the titration. If it is, I might get an O2 monitor with recording capabilities and do some data logging.
Edit: doc called to apologize for hurried appointment this morning and also offered trying an APAP out, thinking the centrals on the study might not be an issue and it would save me another night in a sleep clinic as well as some money.
I agree with the Edit comment. The cost of another sleep study is likely higher than the cost of an APAP purchased on line. A good APAP like the ResMed AirSense 10 AutoSet will clear up the issue of whether or not the centrals are real especially if you review the data in SleepyHead. The only issue is that if it turns out that the centrals are real and significant, an APAP may not be suitable to address them. If it is just a trial and you can return the machine that is ideal. That is the way it works here. They give you a trial machine for a couple of weeks, which you can return. The key here is to carefully review the data from the APAP with SleepyHead.
On the positional stuff, I think the difference you see is quite normal. It is a gravity thing with the tongue.
After reviewing where I am with my insurance deductible and max out of pocket amounts, there isn’t much difference between buying an APAP and getting another sleep study completed. Basically, an APAP will put me into my max out of pocket range (scary, as it’s around 6k), though I can’t really return the machine without paying a substantial fee. I’ve opted to just get the titration study done and be through with it. Hopefully the centrals are mostly about sleep transition and not something more sinister. The doctor didn’t seem too worried about the central aspect as I’m an otherwise healthy and active person.
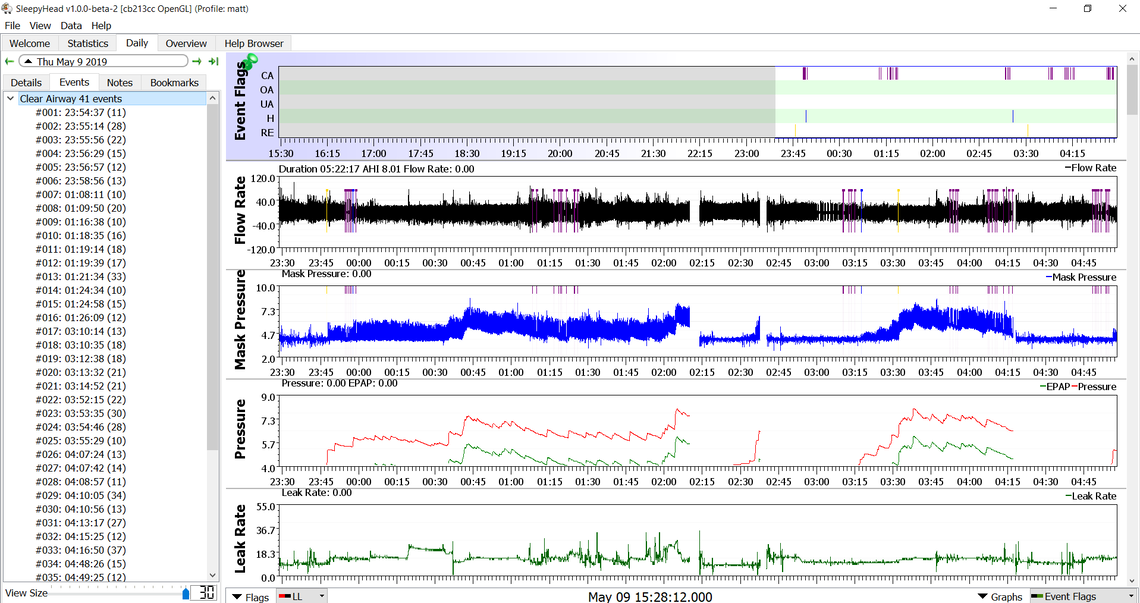
It turned out I wasn’t as close to my max out of pocket as I thought, so I took the docs offer to go with an APAP. Last night was the first night. I wore the mask for about 6.5 hours and had an AHI of 6.3, 6.0 being centrals. However, I was probably only asleep for around 3 hours in total so that score isn’t an accurate representation. I did find myself with some sleep onset apnea a few times last night so I presume some of the score is from that. I copied the files from the SD card to my pc but haven’t had any luck getting sleephead to load them. At this point I’m reluctant to even use the machine again tonight but I’ll want to see what the respiratory therapist at DME says when i get a call back.
Any suggestions on getting sleephead to take my data? Machine is a ResMed APAP 10.
One of the quirky things about SleepyHead is that it seems to want to read the data directly from the SD card. Once you have SleepyHead up and running with the Welcome screen, you should just have to click on the CPAP Importer button. It should find your data on the SD card and ask you if you want to import it. I also use a ResMed AirSense 10 AutoSet and SleepyHead is compatible with that machine.
In general I find if I get a poor sleep I tend to have more central apnea. Some of it is real, but I suspect some of it is what some call sleep-wake junk. SleepyHead will be very helpful in determining what is going on. Some of my highest AHI readings ever was when I first used a CPAP and it was not set up ideally.
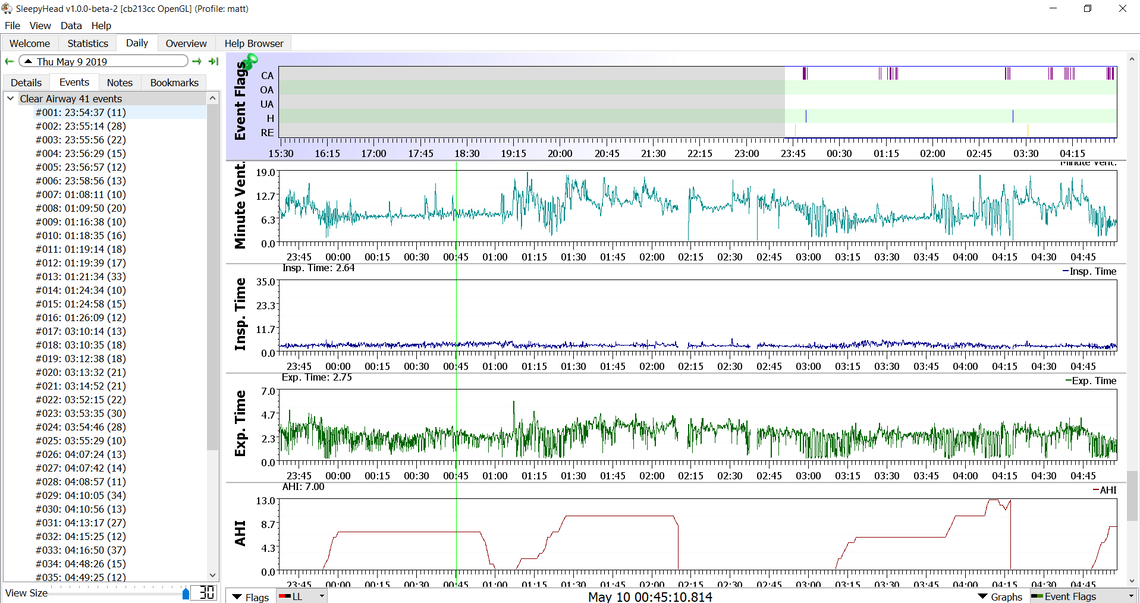
I posted some screen grabs but they aren’t appearing. Perhaps they need to be approved by a moderator first?
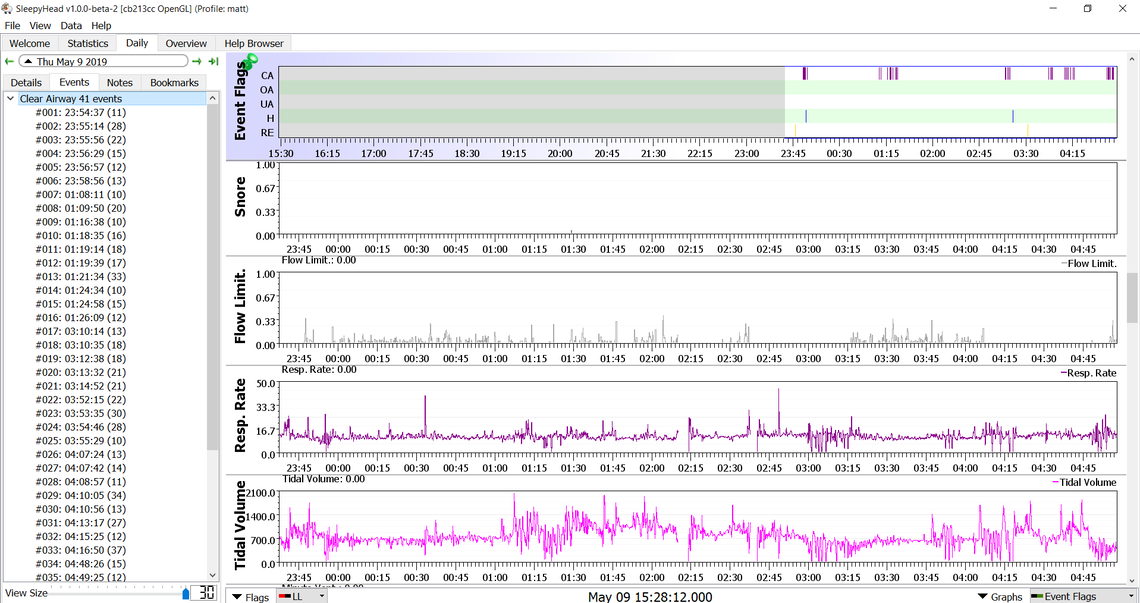
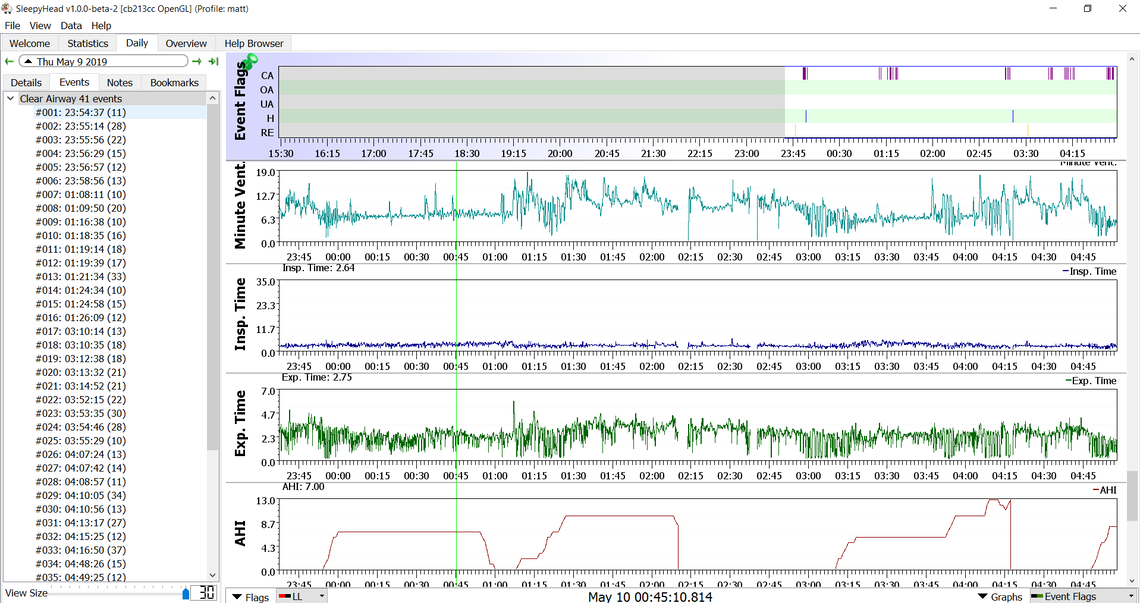
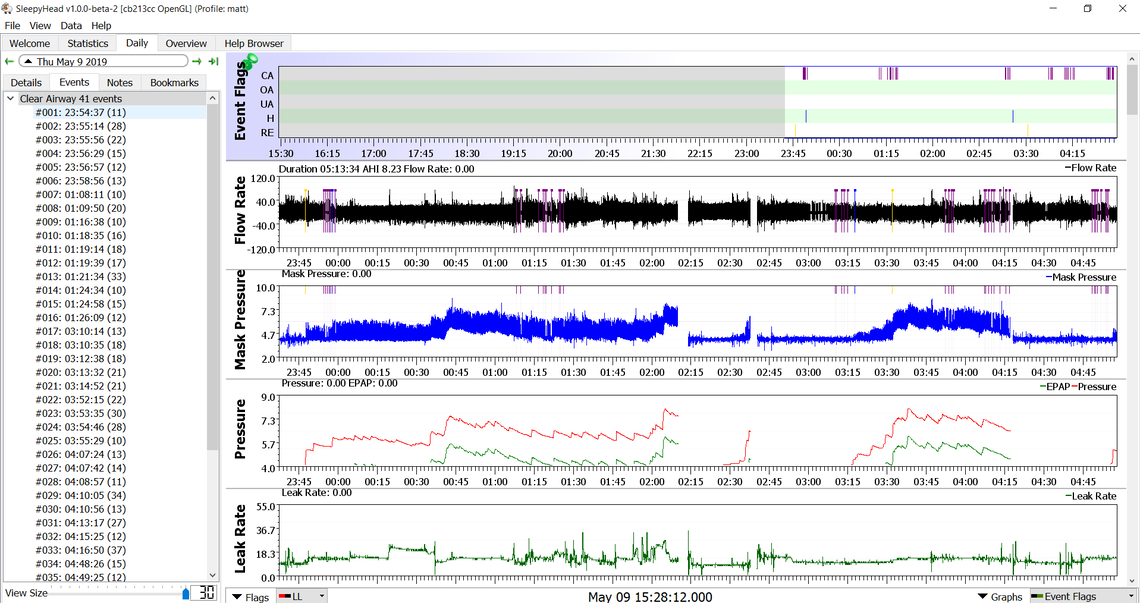
I think if you post multiple graphs in one post they can get caught up by the spam protection software. I would only post one graph in a post. For now that first one with Event Flags, Flow rate, Mask Pressure, Pressure, and Leak Rate is good enough. I would click on the details tab on the left instead of the Events tab. The Details are more important than the event times.
It would be helpful to zoom in on some of those groups of CA events to see what they look like. Put that in a separate post to try and avoid the spam bot. Just keep left clicking and it should zoom in, or use the arrow keys.