How do you get the data of your machine?
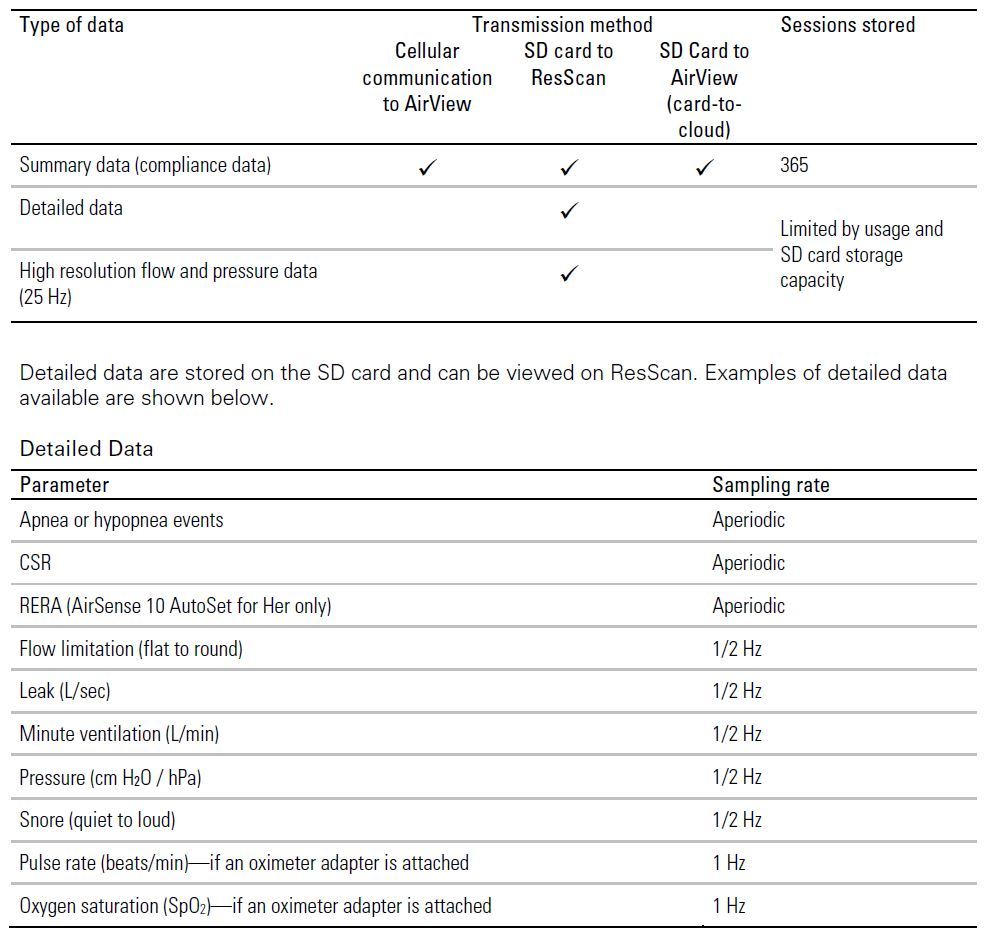
Most new machines use the cell phone network to send information to the machine provider and to the machine company cloud storage (ResMed for example). The data is very limited and mainly intended to monitor and encourage compliance (with using it). The real detailed data is only stored on the machine SD card. This is an example of what is stored where with a ResMed machine.
Why do you need it? Curiosity? Insurance? Do you give it to your doctor? Or use it yourself (it seems bloody complex!)?
Those who monitor their apnea closely need the data to see how well the machine is working and if there are any opportunities for improvement. Some insurance companies use the compliance data to determine if they will take the machine away if compliance is low. No I don't give the data to my doctor. It takes quite a bit of time to review the detailed data, so I expect most doctors just want to look at the summary data. Yes, I look at my detailed data daily to see how well I am doing, what type of apnea I am having, how well my mask is working for leaks. I can also tell if I am opening my mouth in the night causing leaks. The machine will also tell you if anything out of the ordinary is happening -- like Cheyne-Stokes respiration.
And finally is the data you are getting enough?
Yes, when one uses an applications like SleepyHead you can pretty much see all the data you want. If you just use a lightweight application like MyAir, you are pretty much in the dark. But if the AHI is good, and the machine is comfortable, then perhaps that is good enough. For some PAP treatment works very well, and is easy to maintain. For others it can be difficult, and requires pretty constant monitoring..
The main reason for confusion on the part of users is that many sleep clinics try to keep the data from the user, and are not very forthcoming on how it should be set up for comfort. Some even pull the SD card out of the machine before the patient is sent home with the machine. I suspect most sleep clinic technicians do not suffer from sleep apnea and don't use a PAP machine personally. Just my opinion...