CPAP: AirSense 10 AutoSet
Set to CPAP Fixed Mode
Pressure 11 cm
Ramp: Auto
Ramp Start: 9 cm
EPR: 2, Full Time
Mask: ResMed AirFit P10 Nasal Pillow
Canada
CPAP: AirSense 10 AutoSet
Set to CPAP Fixed Mode
Pressure 11 cm
Ramp: Auto
Ramp Start: 9 cm
EPR: 2, Full Time
Mask: ResMed AirFit P10 Nasal Pillow
Canada
Sounds like they are playing a little difficult with the sleep report. I would suggest you make an appointment with your doctor, ask to see the report, ask for his/her opinion as to what it means, and also ask for a copy.
My wife and I are now both on a CPAP. She was diagnosed nearly 4 years ago in the high severe range - around 80 I think. When she went on the machine she noticed an immediate benefit, and has used it every night since getting it. I was tested after I failed a screening test and then failed the sleep test with an AHI in the lower severe range - 37. I had no trouble sleeping before the machine, and did not suffer from any extreme sleepiness. So I did not see an obvious step change. Now after 6 months I am seeing more benefit. My wife's apnea is essentially all obstructive apnea and she averages about 1.0 for AHI under treatment. I am doing well to get under 3.0 due to my higher portion of central apnea. My wife also appreciates that I no longer snore too!
I did a quick check on BC's health care treatment of apnea. It is better than Alberta. We have to pay for our machines out of our pocket if we do not have private insurance plans that pay for it. I see in BC that if the severity is moderate (AHI 15-30) or severe (AHI >30) it looks like they pay. But, you may be on your own for cost if mild (5-15). We had to pay for our machines, and there is a wide variation in what they cost depending on where you get them. I can help you out with some suggestions on where to go for a better price if it comes to that.
In any case step one is to get your sleep report(s). That will provide a lot of guidance on what you are up against, and what your options may be. There are at least 5 different types of central apnea, and various types of treatment methods depending on the type you have. Here is a short report on it, if you have not seen it before.
Central Sleep Apnea
Oh and the other important part of the sleep study report is the oxygen desaturation levels. The problem is not really that we stop breathing, it is that oxygen levels go down when we stop. That causes the problems. The report should say to what degree that is a problem for you.
Hope that helps some,
I am from Canada and understand what you are dealing with to some degree. I have had the home sleep study and the results indicated a small degree of central apnea. My results:
Type - Index (#/hr)
Central - 0.4
Obstructive - 17.4
Mixed - 0.7
Hypopneas - 18.8
Total - 37.3
That puts me in the severe classification (AHI > 30)
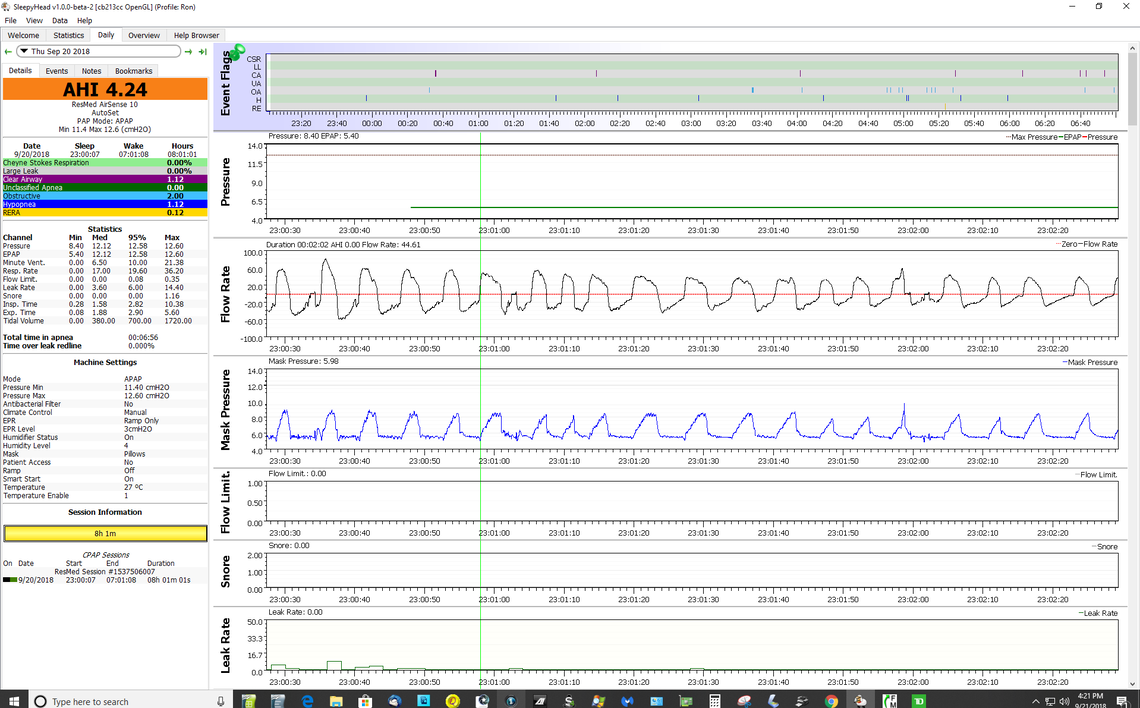
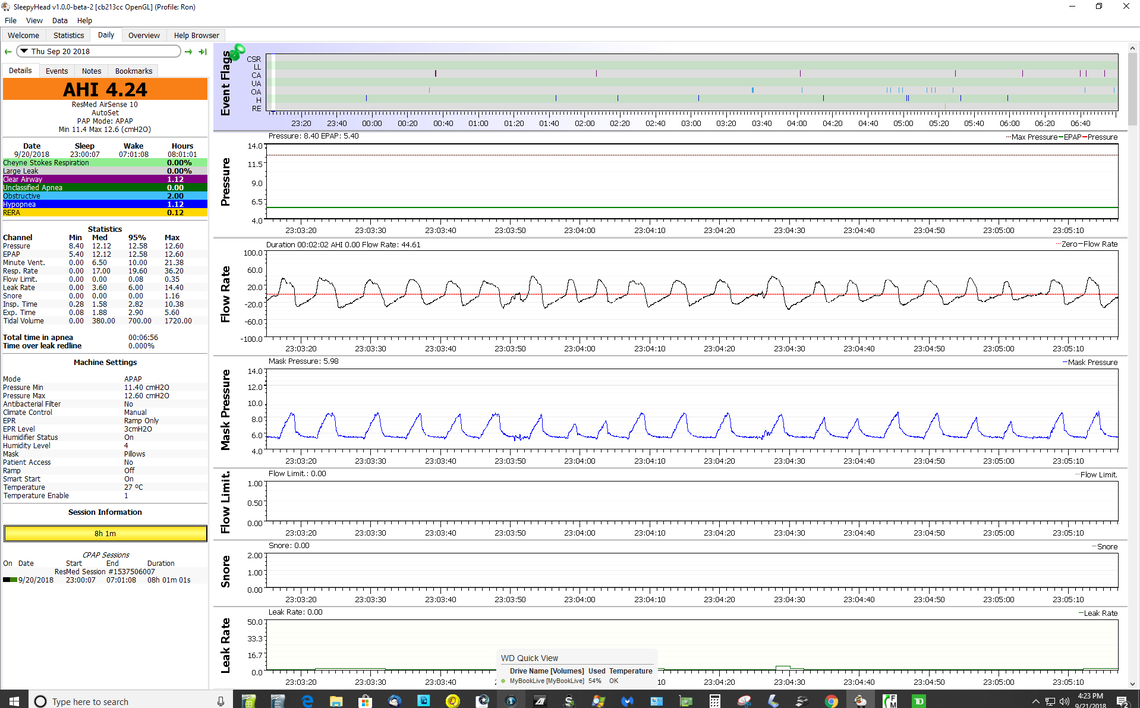
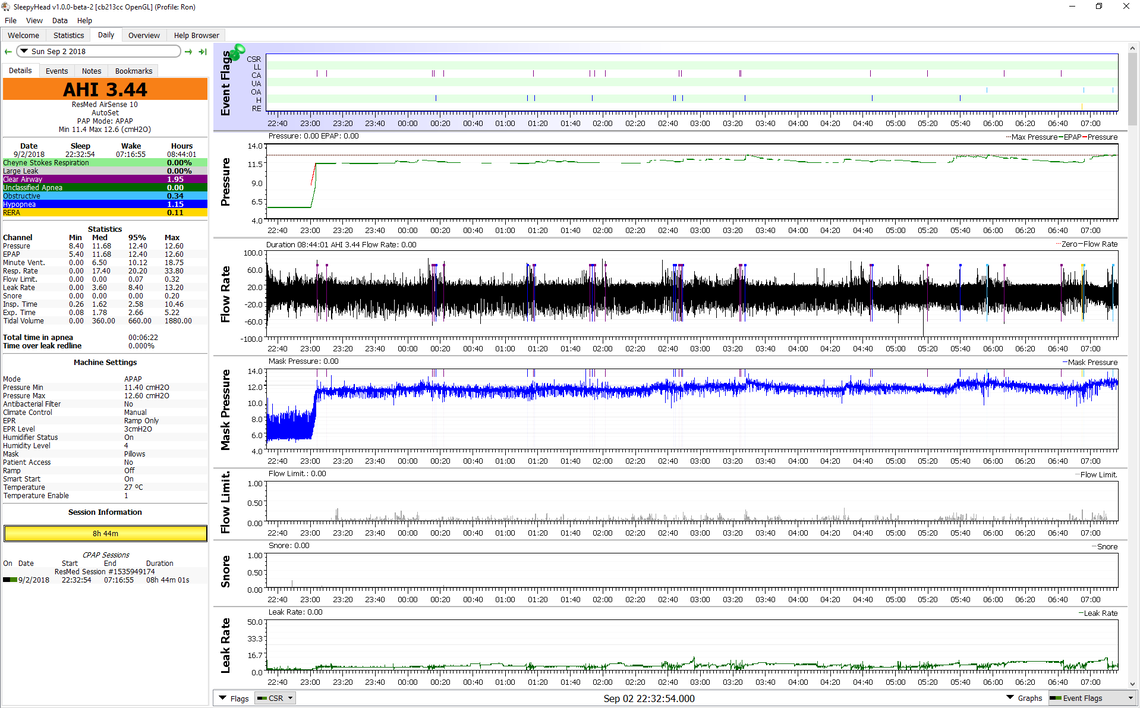
My issue has been that Auto CPAP treatment has significantly reduced the Obstructive apneas, and Hypopneas, but the Central apneas have increased. Under treatment my total AHI is about 3 with the largest portion being central, then hypopneas, and lowest are the obstructives. The hypopneas are probably partial centrals, so Centrals is likely a little understated. This said one is considered to be adequately treated if AHI is under 5.
To access your situation you need to get these kind of numbers. Ask your sleep test provider to e-mail them to you. They probably have them electronically already, or can scan them. If they won't, then ask your referring doctor to provide them. I don't believe they can refuse you, and you deserve to see the results.
When you get the results then you can start to assess the seriousness of your condition. It may not be bad at all. If you can post your numbers then I certainly will comment on them. I am not a doctor, but as centrals have been an issue for me, I have done a bit of research on it. If you have obstructive apnea to be treated, there is only so much a standard Auto CPAP can do. A BiPAP machine can do a little more, but not much. The ASV or ventilator machine can do more, but they would probably only be used if there were no other options to treat the underlying conditions.
Short story. Insist on getting a copy of the sleep report; both the first one and the second one. Do you know the name of the machine you used? ResMed make one called ApneaLinkAir, and Phillips make one called Alice NightOne. I had my test done with the NightOne. The link below is to the product brochure for the ResMed machine. See page 4 for an example of what the sleep report from it looks like. That is the report you want to get. There should also be a professional evaluation of the results and their comments should be included as well.
ApneaLinkAir