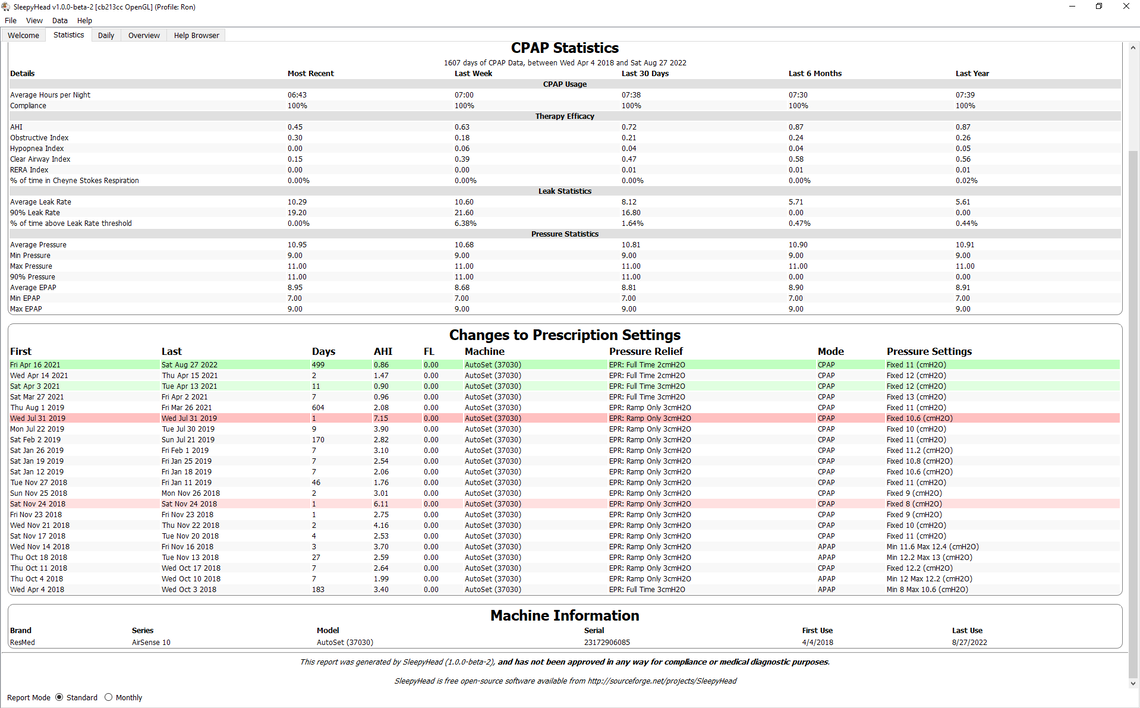
CPAP: AirSense 10 AutoSet
Set to CPAP Fixed Mode
Pressure 11 cm
Ramp: Auto
Ramp Start: 9 cm
EPR: 2, Full Time
Mask: ResMed AirFit P10 Nasal Pillow
Canada
CPAP: AirSense 10 AutoSet
Set to CPAP Fixed Mode
Pressure 11 cm
Ramp: Auto
Ramp Start: 9 cm
EPR: 2, Full Time
Mask: ResMed AirFit P10 Nasal Pillow
Canada