We also have both, a Resmed Airsense 10 like yours and a Dreamstation-1 APAP which my wife uses for he OSA. (and no, she does not use the "FOR HER" feature of the Resmed for good reasons...See below)
She finds the difference between the 2 machines, like night and day in that she now refuses to use her Resmed altogether.
1- Resmed Airsense algo does what Resmed wants to do, not what the patient wants it to do and thus its response to patient comfort is very limited, even when the EPR is turned on, where as according to my wife, she doesn't even know she is wearing a mask when she is on her DS-1.
That is because Dreamstation algorithm to treat OSA is not only more responsive during inspiratory-Expiratory transition, but also much smoother in when changing pressures, unlike Resmed which according to her tends to have a much sharper (jerkier)n transition. so it is not that DS is "slower" than Resmed but that the DS algo makes the transition between IPAP and EPAP a lot smoother so patients can't feel the change with Dreamstation patented C-Flex technology..
2- Resmed's Auto PPAP algio essentially fakes mask pressure on data because they do not have separate sensors for the mask pressure built in, so they just derive this from calculation. The displayed mask pressure therefore is hypothetical, not an actual one, so I wouldn't place too much emphasis on that feature.
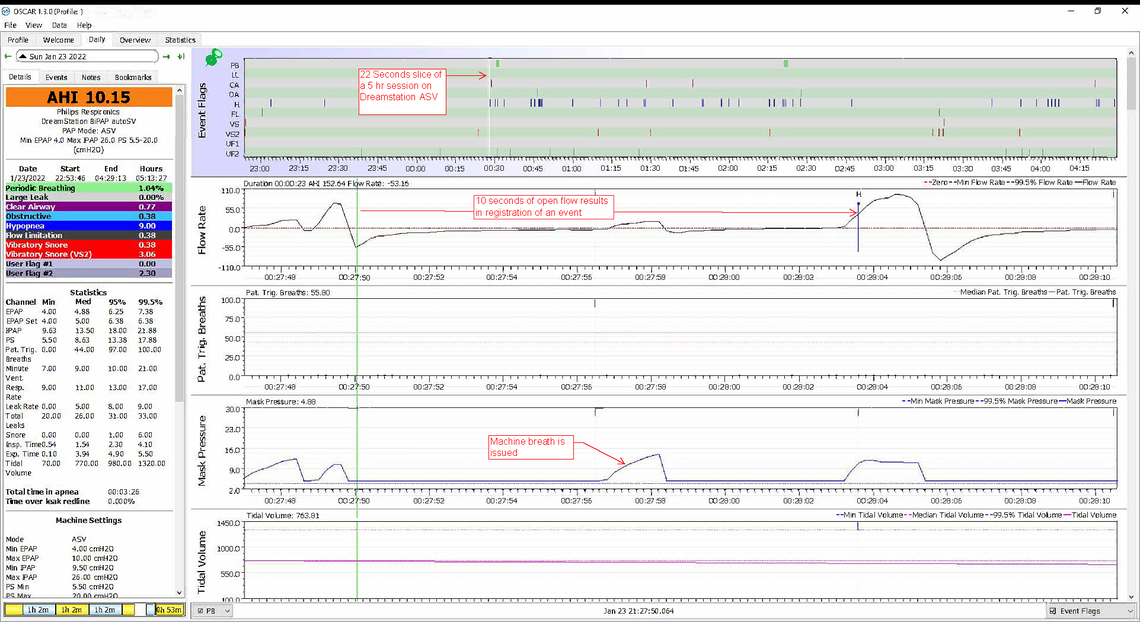
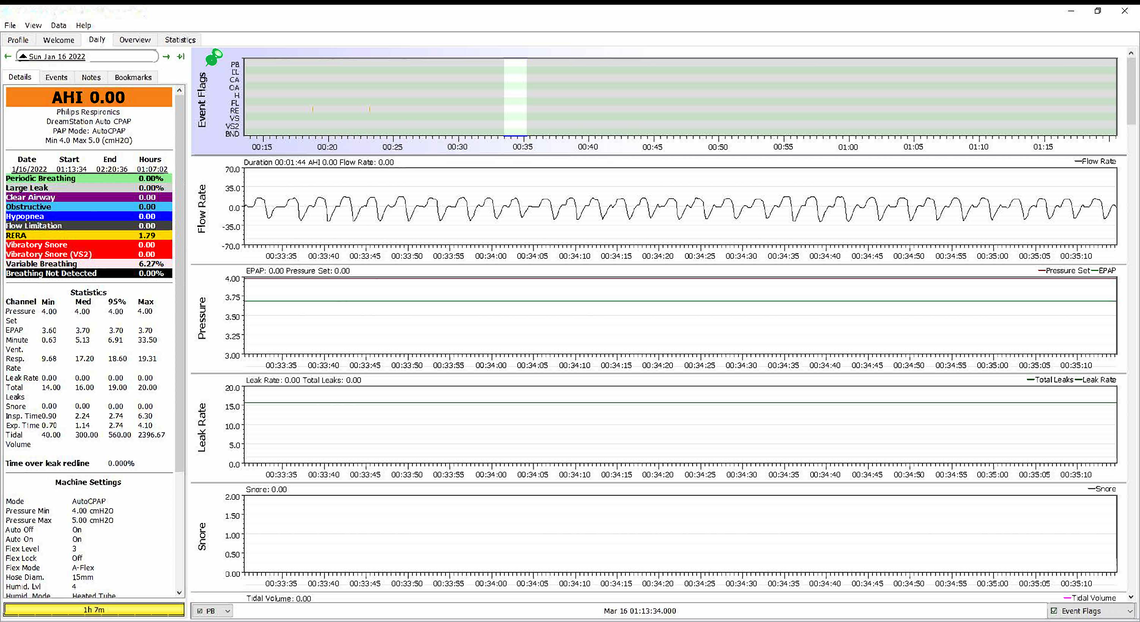
3-In contrast, Dreamstation-1 APA reports FLOW rate, precisely measured as you can see in my wife's chart. Her flow rate is perfect breath by breath, in comparison to your Airsense chart which reports a flow rate that is far from perfect, not necessarily because you are not breathing well naturally, but because you are not breathing well BECAUSE of Resmed's faulty pressure delivery. Worth looking into.
4-"For Her" algorithm that Resmed keeps coming up with (yes they have them on their latest model 11 too), is more of a sales gimmick than it is a real medical feature.A pap machine algo should respond to one's respiratory needs, regardless of their gender. Dreamstation machines algos are "Gender-Blind" and this even more "politically correct":-)
5-Her Dreamstation also has all the comfort settings that her Resmed has, including a cool Ramp feature that truly "RAMPS" the pressure up over the period that ramp has been set to, unlike how Resmed controls Ramp which at times jolts her awake.
Ramp function should be true to the meaning of the word, a linear increase in pressure, divided precicely over TIME setting, which is what Dreamstation delivers.
At any rate, as the original inventors of PAP technology and their sizeable investment into the development of these essential medical devices, it is natural that Philips-Respironics software has been worked on a lot longer and naturally at a much deeper level than Resmed systems.
Problem here is Resmed algorithm clearly does NOT recognize clear apnea events and ignores them, thus reporting a much lower AHI while not delivering full therapy.
This is simply wrong .