I copied my previous response to you on EPR below. I won't repeat that part again. What is new is your question about leaving EPR on full time. The problem with EPR is that it reduces your exhale pressure. Apnea can occur on inhale or exhale or the transition from one to the other. If for example you have a set pressure of 8 cm and an EPR of 3 then all night long the pressure will cycle from 8 cm to 5 cm on each inhale and exhale. If you are susceptable to apnea event on the transition or during exhale your effective treatment pressure is only 5 cm. But, you are having to endure a pressure of 8 cm on inhale. You may get almost the same benefit in apnea prevention by running a fixed 5 cm pressure.
The short story is that if you want to know what your effective treatment pressure is, then you have to subtract the EPR value from the set pressure. And if a set pressure of 8 cm and EPR of 3 works for you and feels comfortable then leave it that way. It indicates you really only need 5 cm, but that does not matter much. What works for you works for you.
" EPR stands for Expiratory Pressure Relief. It causes a reduction in the mask pressure when you breath out compared to when you breath in. The number is an approximate pressure reduction in cm of water pressure, often just called cm. Let me give an example:
If your therapy pressure is set at 8 cm, and you have EPR set at 3 cm and is turned on, then you will get 8 cm of pressure when you breath in. And you will get 5 cm (8 less 3) when you breath out. Now if you have a set pressure of 4 cm and and EPR of three, the EPR tries to reduce pressure to 1 cm on exhale. However, the machine is designed to never let pressure go below 4 cm. So in that situation the EPR does nothing. You will get 4 cm on inhale and exhale.
So if you set it up with the ramp in auto, a start pressure at 8 cm, and EPR at 3 for ramp only, it will go through this sequence. When you are still awake it will give you 8 cm on inhale, 5 cm on exhale. Most find that very comfortable. Then when you go to sleep, it will stop reducing the pressure on exhale. Most do not notice this change when they are asleep.
There is nothing magic about setting the ramp start pressure at 8 cm. If you find that too high, then try a ramp start pressure of 7 cm. Then it will do 7 cm on inhale, 4 cm on exhale, and then ramp up to a constant 8 cm when you go to sleep. The problem with setting the ramp start at 4 cm is that most people will find that too low, and feel like they are suffocating. I personally have a ramp start at 9 cm. I find that very comfortable, but everyone is different. Most with experience prefer a high pressure. A higher inhale pressure makes it easier to breathe.
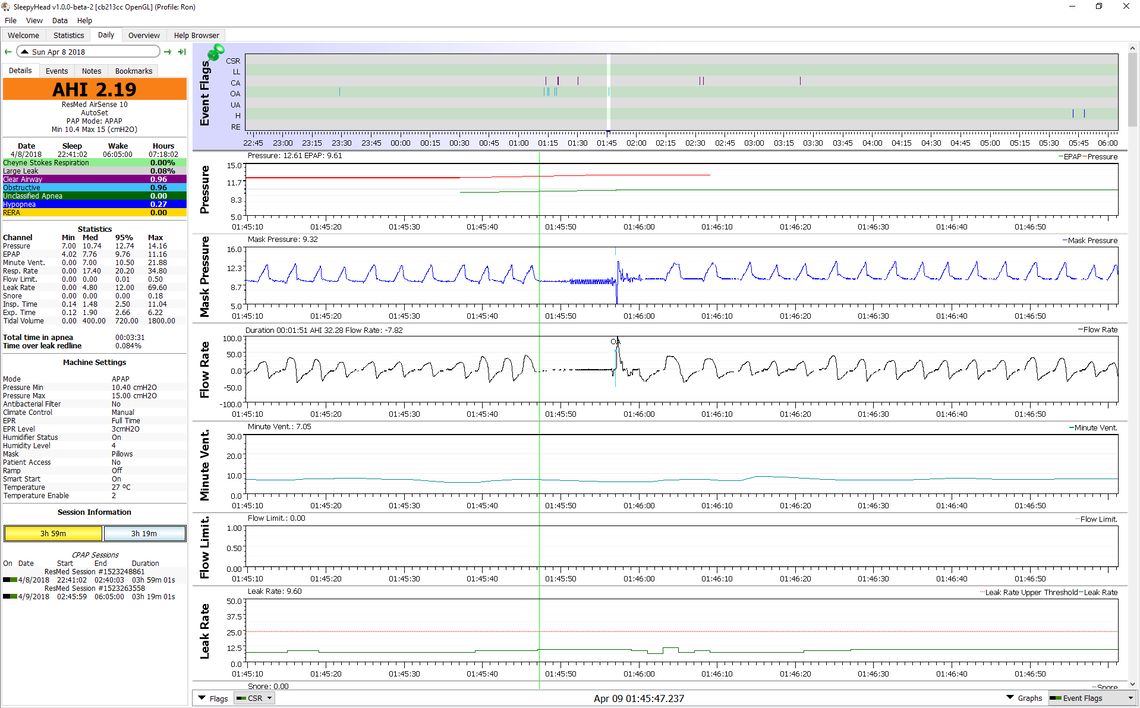
Here is an example of how my machine works, as shown with SleepyHead. This is with an auto ramp, a ramp start of 9 cm, EPR at 3 cm, for ramp only, and a therapy pressure of a fixed 11 cm. You can see how mask pressure cycles between 9 cm and 6 cm for each inhale and exhale. Then when breathing becomes regular and it detects I am asleep (about where the green line is) the pressure ramps up from 9 cm to 11 cm, and then finally stops the reduction on exhale.
You asked whether 8 cm was a high pressure. My opinion is that it is a quite low pressure. Your machine has a maximum of 20 cm. Some machines go up to 25 cm. So if you think 8 cm is a lot, consider that some are using three times that amount."
Hope that helps some.