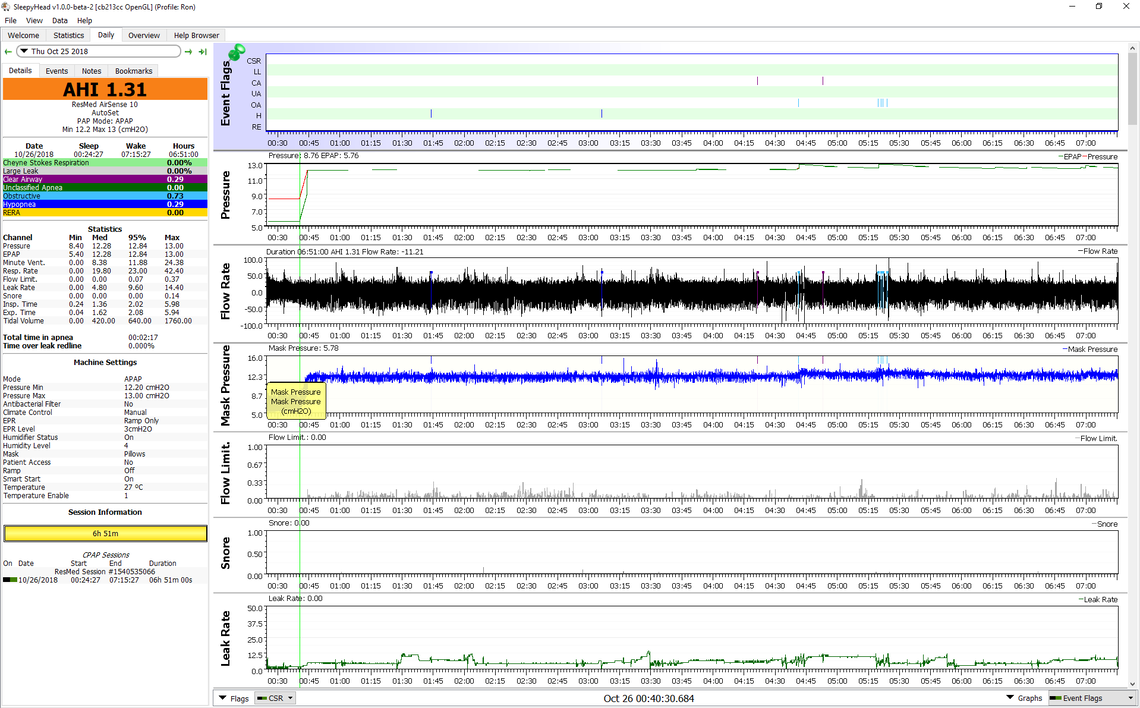
The good news here is that CA is still zero. It is possible the hypopnea events are central apnea related though. You would have to zoom in to see what they look like.
Some things to keep in mind in this. You have made very rapid progress, and are now at the point of making some pretty small changes. When you make a small change, you probably have to try them for a week or so before you can be sure what effect they have. It is kind of like changing the brand of your golf ball, playing one hole, and then trying to decide if it is better or worse. I have been averaging about 2.3 AHI for some time now with my latest settings. Last night it was 4.3. I had changed nothing other than we added a quilt for the winter and it may have been too hot...
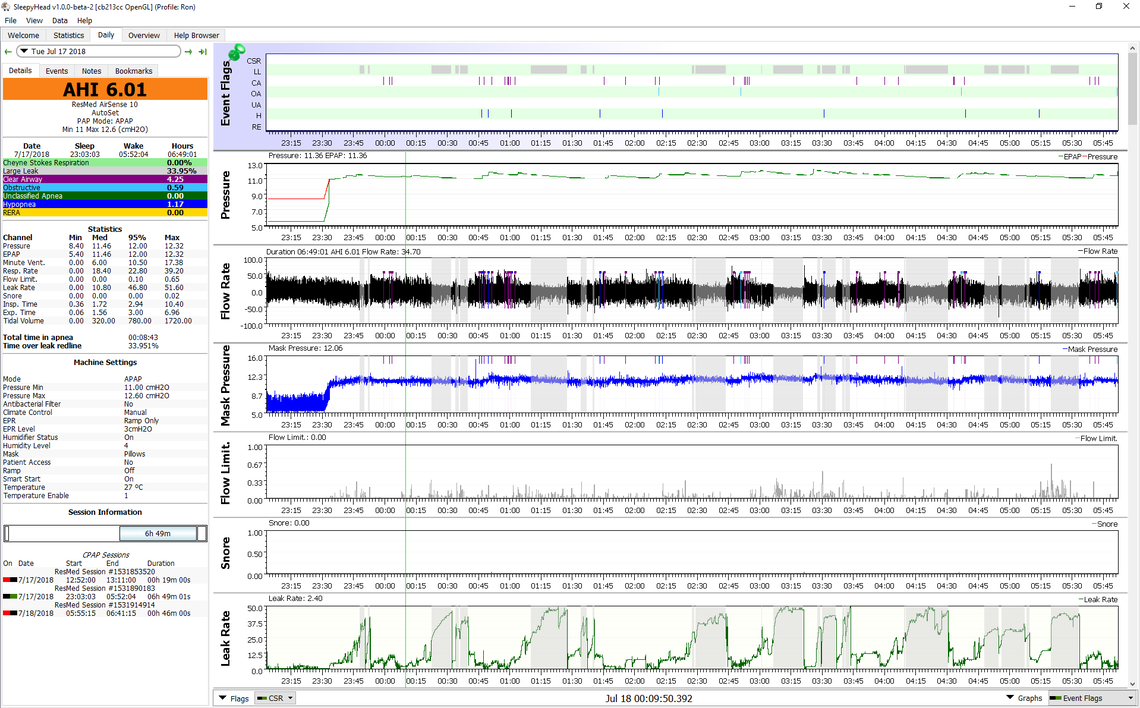
In general your CA is zero so that suggests at first blush that pressure is not too high. Your OA is 0.69 which all considered is pretty good. That suggests your minimum pressure is not too low. The only remaining issue is the hypopnea. I would be suspicious that along with another green band of PB indicates central apnea may be at work but not just causing a full CA. I have to admit that when I see CA low and OA low, I kind of ignore the hypopnea, or at least give it a lower weighting for concern.
I see you have moved the AHI graph up. I find that graph somewhat misleading and not all that useful. My preference is to look at each event and see at what pressure was there before it occurred. That is why I put the pressure graph right below the events, and mouse over the cursor to see the digital display of pressure above the graph. It tends to be more accurate than trying to read the graph directly.
You said "So my opinion is a range from 9.0 Epap to 10.0 Ipap, with 1 Bi-Flex, is where our next test should be."
I think that is as good a setting as any from what I have seen so far. It would be worth trying that for a few days without making any other changes to see what it produces. Perhaps just leave the settings at that and post your daily screen each day to see if there is any kind of trend to the results before making any other changes.