First, I have to say you are doing an amazing job in tracking your progress and keeping the detailed spreadsheets. In looking at the spreadsheets a couple of things jump out to me. First since Feb 28 when you increased maximum pressure to 10.4 cm the OA frequency with the exception of one night has been really good. The average is under 1.0. This suggests to me that 10.4 cm is probably enough to control most of the OA events. The second thing that jumps out is that when you were using the S9 machine with EPR at 3 cm full time your Hypopnea was much lower and looks like it is well under 1.0 compared to nearly 2 now with EPR on ramp only.
Putting this together this is what I would do. First switch the machine to fixed pressure CPAP mode. You are spending very little time at less than the maximum pressure, and gaining very little with increasing minimum pressure. You may as well go to one fixed pressure that you can control. My suggestion based on your spreadsheet data would be to try 10.4 cm for the single fixed pressure. I would try that for a couple of nights just to confirm what it does. And next I would switch the EPR to Full Time with it set at 1.0 cm. Then if everything looks OK, increase the EPR to 2 cm and then 3 cm to find out if that will reduce the Hypopnea. The objective would be to only use enough EPR to reduce the Hypopnea but not increase the OA frequency.
And then after you determine the optimum EPR (the minimum you can get away with), then you could try lower fixed pressures to see what pressure you can get away with, without OA events going up. You may be able to get away with less than 10.4 and less might reduce the CA frequency.
You asked about sleep quality and I am a poor one to ask. I was diagnosed with an AHI of 37 or so, and next to zero CA events. But with treatment the CA problem emerged. And before diagnosis I was sleeping well (but snoring!). So, I did not see a big improvement in sleep quality, but I'm sure my wife appreciates the reduction in snoring. On the other hand, my wife was diagnosed at an AHI of 73 or so. Her treatment has brought her AHI down to 0.6 and she says she has an amazing improvement in sleep quality. But, I think my sleep quality is better than hers. She insists on having daily naps while I do my best to avoid naps during the day and try to sleep between 7 and 8 hours each night.
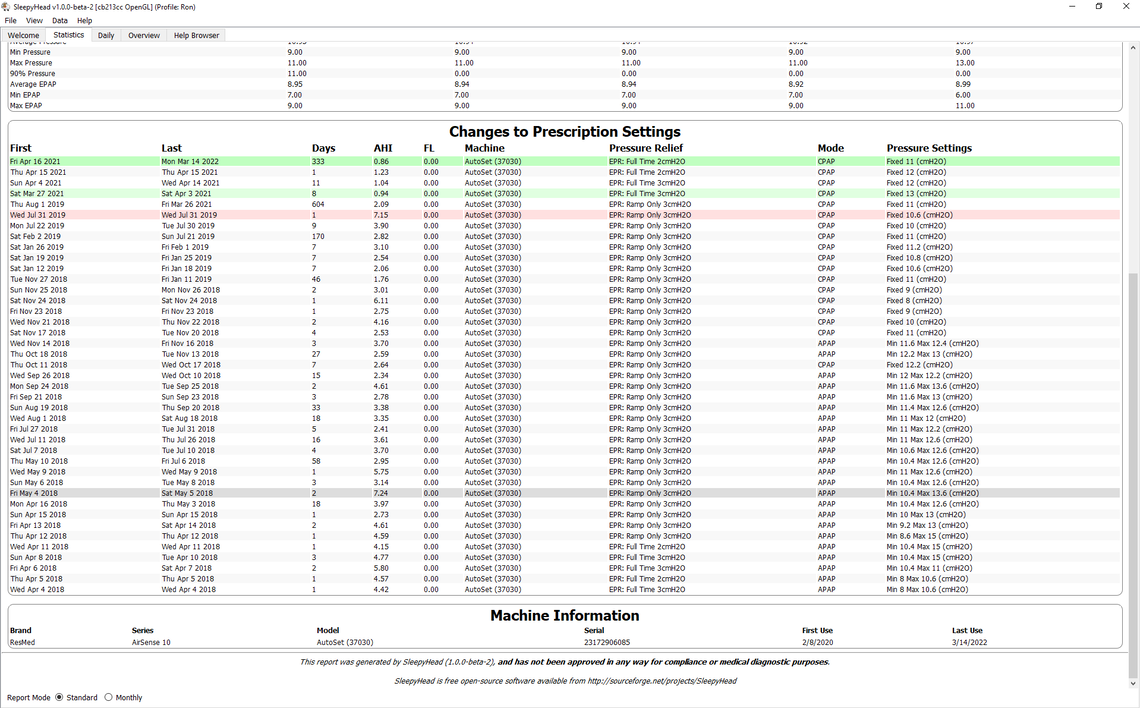
To give you some idea what it takes to get the machine optimized here is a screenshot of my statistics since day 1 with my A10 machine back in 2018. I kind of went through phases where I reduced the gap between min and max pressures. and then switched to a fixed pressure with many attempts to determine the best tradeoff pressure, and then finally to try EPR at 2 cm. I should probably try EPR at 1 cm but have not done that yet. As you can see, it is a long and winding road to get to some kind of optimum setting.