Written by Gail Demko, DMD, Expert Advisor to the FDA and Associate editor of the Journal of Dental Sleep Medicine
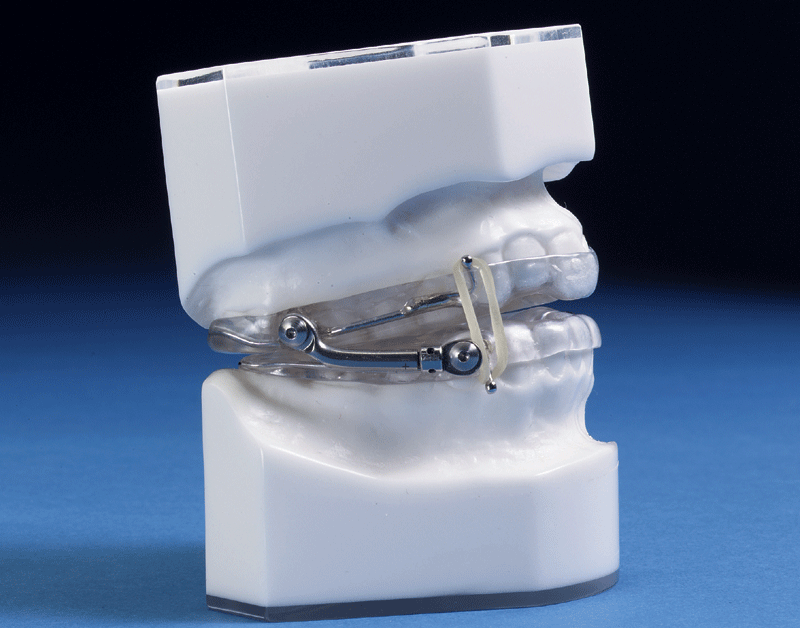
Oral appliance therapy for obstructive sleep apnea has existed for almost 35 years. The most common oral appliance moves the bottom jaw forward so the bottom front teeth are level with the upper front teeth. To do this, the appliance uses the upper teeth as an “anchor” to move the jaw forward. The device looks like two dental retainers connected with a hook, a bar, a strap or some other connector. The FDA has cleared more than 100 oral appliances for treating snoring and obstructive sleep apnea.
How oral appliances work: The idea of using oral appliances to move the bottom jaw forward come from work done in 1909 by the German orthodontist, Emil Herbst. Orthodontists began using these devices as “functional appliances” in the 1970s. These functional appliances were developed to move the jaw permanently forward in young patients with an undersized lower jaw. Appliances work because the tongue and the sides of the throat are attached to the bottom jaw. When the bottom jaw is moved forward, the tongue moves forward too and the sides of the throat open the upper airway sideways. This treatment often works well for patients who have sleep apnea largely due to having a small throat size. Those patients have too much soft tissue in too small an area or have a highly collapsible airway (throat area). Oral appliances do not work for everyone. Research consistently shows that only 50% of patients who get oral appliances can totally control their sleep apnea with this treatment alone.
Role of oral appliances in treating sleep apnea: Even though there are drawbacks to using oral appliances, patients often prefer them to using CPAP. While the devices may be less effective in eliminating breathing pauses (apneas) than CPAP, many patients report using the devices for more time at night than CPAP. Some research shows that over the long term, oral devices may improve many symptoms and signs of sleep apnea. Many people who travel a lot find benefit in using these devices. Young people often prefer them because of their social situation (living in a dorm or dating).
Possible side-effects and precautions: These devices are not usually used in patients younger than 18 who may still have a growing jaw bone. They also have the possible side effect of permanently moving an adult patient’s jaw forward. Since the teeth are used to anchor the oral appliances, tooth movement may also happen. Side effects are normally small, and often do not impact function. But, when the patient is not working with a qualified dentist, the side effects can become quite pronounced. Remember: all medical treatments have side effects. Obstructive sleep apnea is a serious disease that can increase risk for sleepiness related accidents, high blood pressure, and other health problems. Patients with sleep apnea should be followed by their health care providers to make sure their disease is being well treated.
Work with a dentist to find a safe, comfortable device: Because there are side effects, especially in young people, it is important that oral appliances are only used with the supervision of a qualified dentist. A dentist well-trained in treating patients with sleep apnea understands that adjustments to the appliance are needed if the teeth start to shift. Research studies have shown that patients are totally unaware of changes in tooth position until the changes are very advanced. A trained dentist would be able to detect these changes in time to adjust the device and prevent major problems.A properly adjusted oral appliance is not uncomfortable. A qualified dentist must adjust any appliance to find the proper fitting, even for devices available over-the-counter. If an oral appliance is uncomfortable, it is not fitted correctly. Custom fitted appliances made by a qualified dentist are twice as effective as oral appliances that are bought online or in-store. The main advantages of custom fitted appliances are that they are more comfortable, they do a better job of holding the bottom jaw forward, and they have a longer life-span. If you were successful with an appliance you fit yourself, then an appliance made by a qualified dentist will also be successful. If you were not successful with an appliance you fitted yourself, this does not automatically mean a custom fitted appliance will fail. Also remember: medical insurance only pays for custom fitted oral appliances.
Oral appliances and CPAP: Oral appliance therapy may be used with CPAP to improve treatment. Alternating between using CPAP and an oral appliance is an option for those who remove their CPAP mask in the middle of the night. A lot of research has tried to find out which patients respond best to oral appliances. Unfortunately, there is no answer yet. So, it is generally recommended that most people with obstructive sleep apnea try CPAP first. This is because CPAP is currently the most effect treatment for sleep apnea. However, oral appliances are the second most effective treatment and could be a good option for many patients who do not tolerate CPAP well. Since oral devices are covered by all major medical insurance providers, even Medicare, you can freely choose your treatment, guided by a discussion with your sleep physician, the level of your sleep apnea, and your dental condition.
For help finding a qualified dentist, you can ask your sleep physician or you can go to the website of the American Academy of Dental Sleep Medicine.
The question of the role of oral appliances for sleep apnea treatment is important. There are research studies examining the effect of oral appliances on symptoms (sleepiness, alertness, sleep quality) and long-term health problems, such as high blood pressure. We need more research to learn how patient feedback and preferences can help guide sleep apnea treatment plans. Let us know your thoughts: how can doctors and dentists work with patients to better understand how to treat sleep apnea?