Thanks
I am on PC, Windows 10 32-bits.
Here are some more points.
1.The term AHI is, from what I understand, an umbrella term including a variety of apnea events, like O.A, Hypoapnea, Central Apnea and others.
To be able to identify them individually is essential, but if Resmed, to this purpose, removes the AHI’s from the report in case of large leaks, will these individual apnea modes be still traceable? If not, won’t the reports be unreliable, if they don’t show the correct number of AHI events?.
It is a bit like deleting a folder from the computer: all the files it contains will also be gone.
- Your comments have been invaluable, also because they have led me to look into the differences between the various apnea events, like Central Apnea, Obstructive Apnea, Hypoapnea, etc.
I don’t have, though, a clear appreciation of their impact on the patient’s sleep quality and, ultimately, on his/her health. .
I’d would think that OA has perhaps the greatest impact, but perhaps other apneas are just as important..
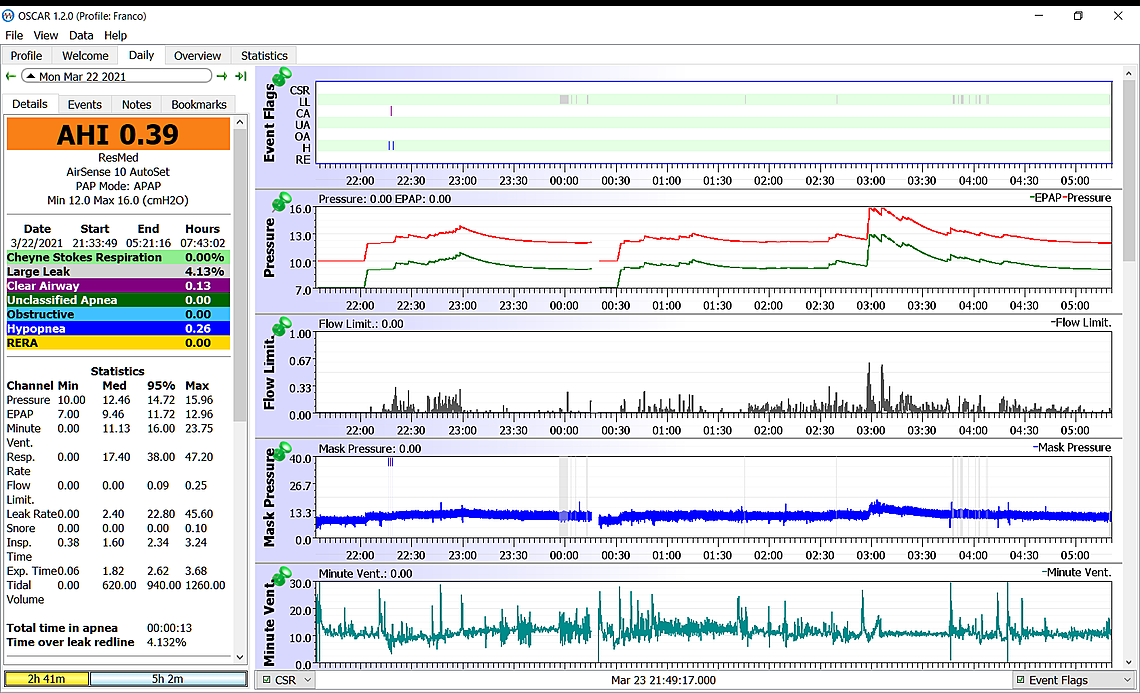
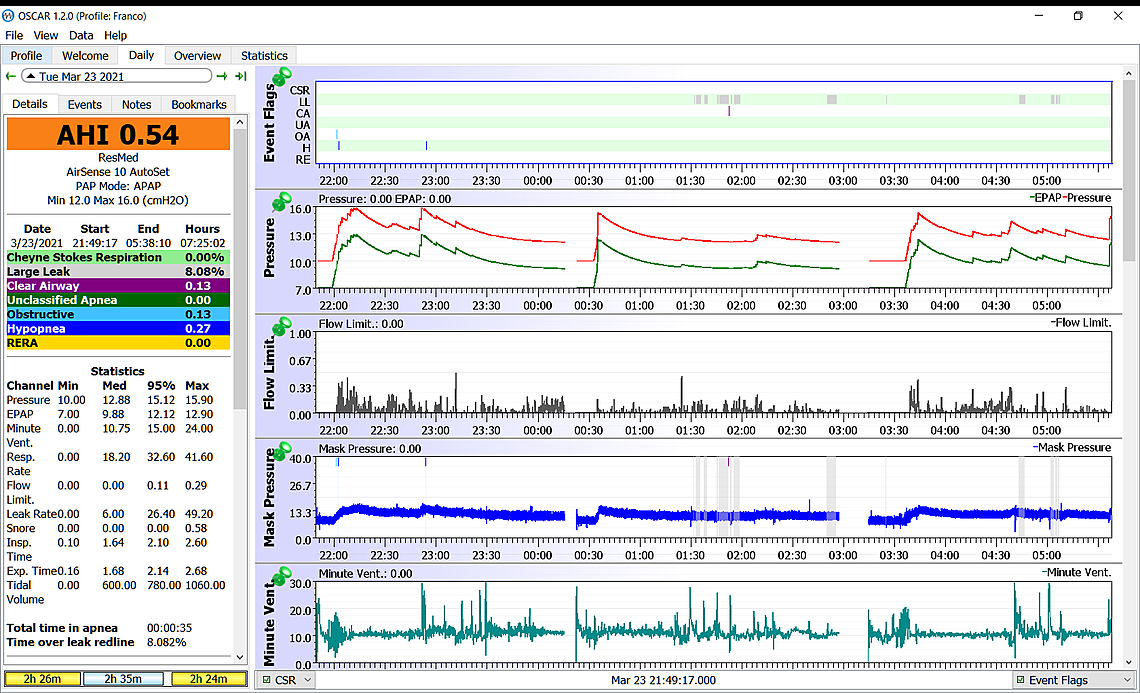
My AHI’s have drastically gone down, in the average, to well under 2 /day over one year. . Sometimes there is none and sometimes, very rarely, they spike to 6-8 in one night.
Looking at my reports, I found that the OA’s represent about half of my AHI’s. and this raises a few questions.
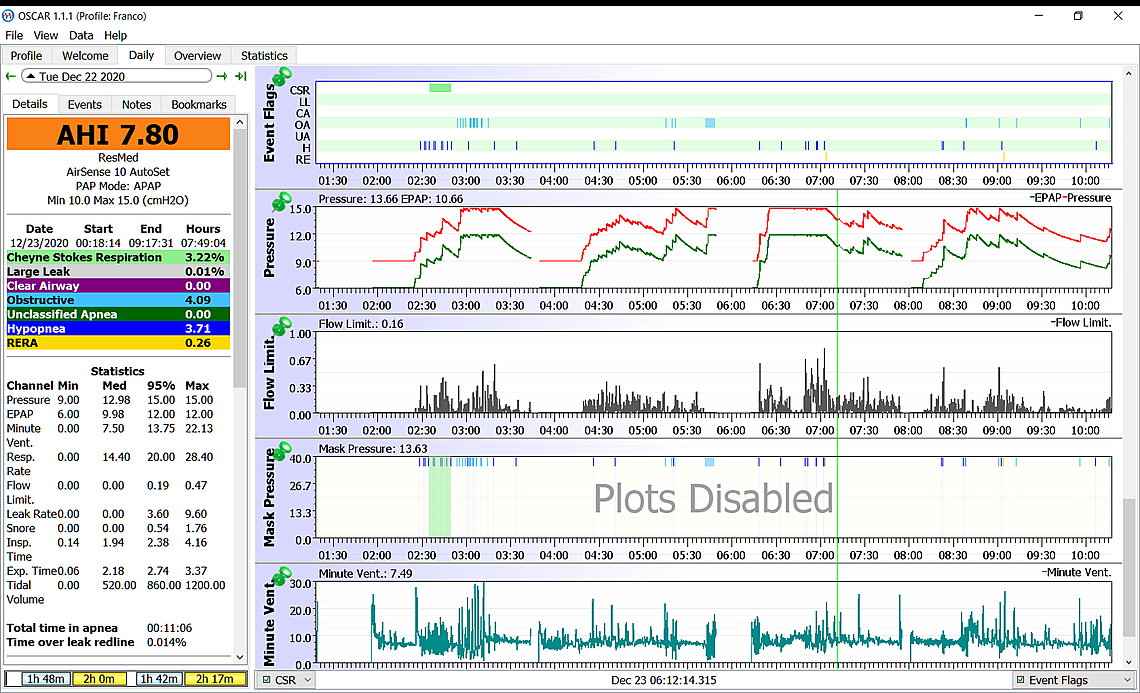
Of course, if the AHI’s for the night are down to one or less, the OA component becomes insignificant. When, however, the AHI’s are six or eight and half of them are OA’s, I wonder if there isn’t a more serious impact on health.
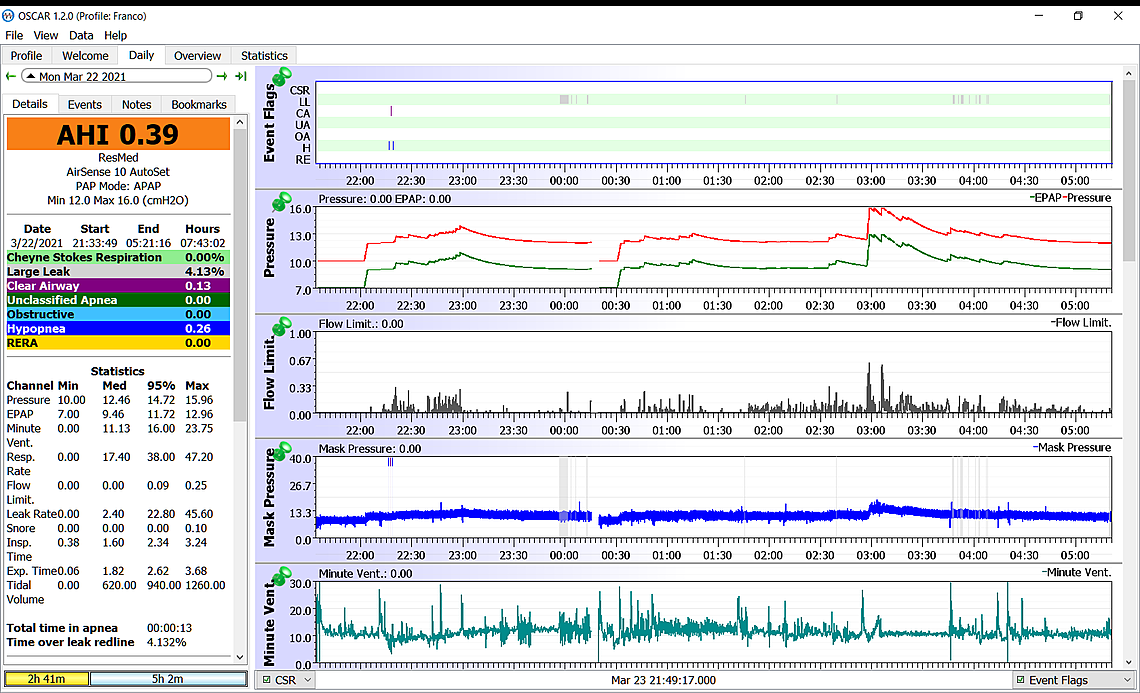
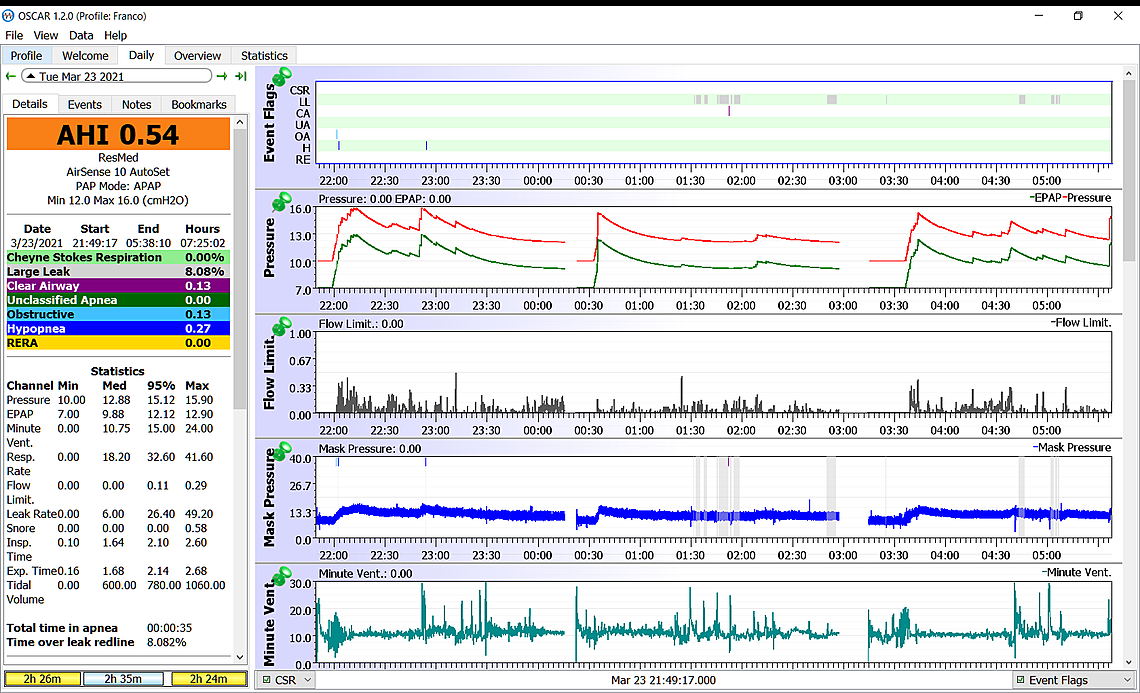
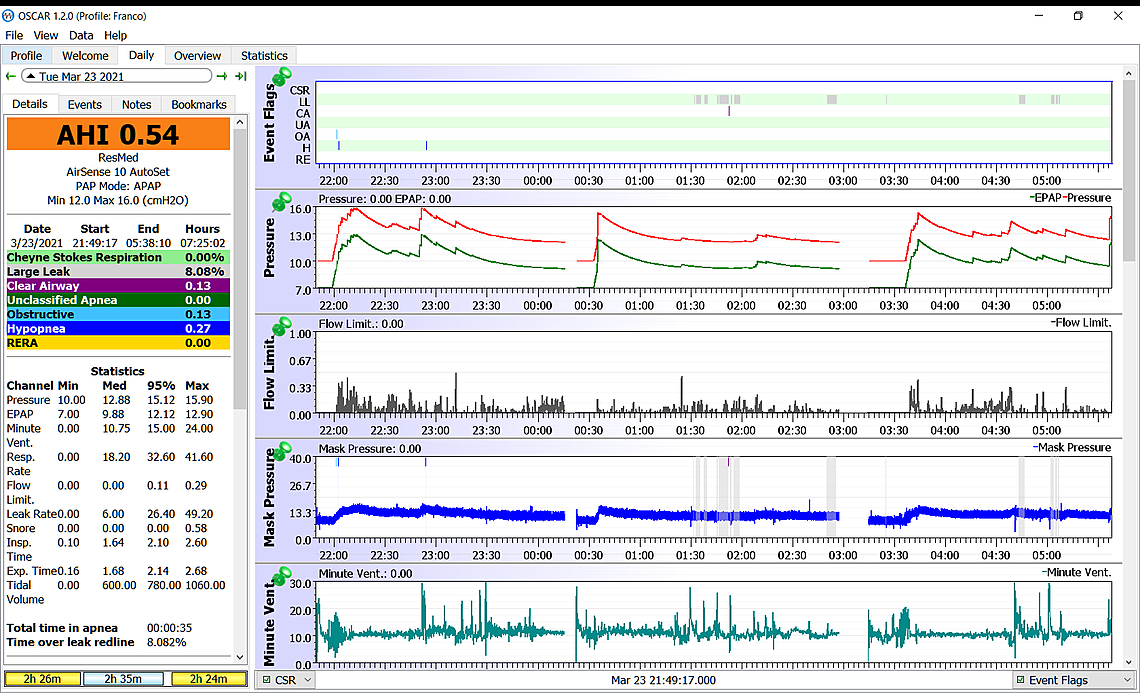
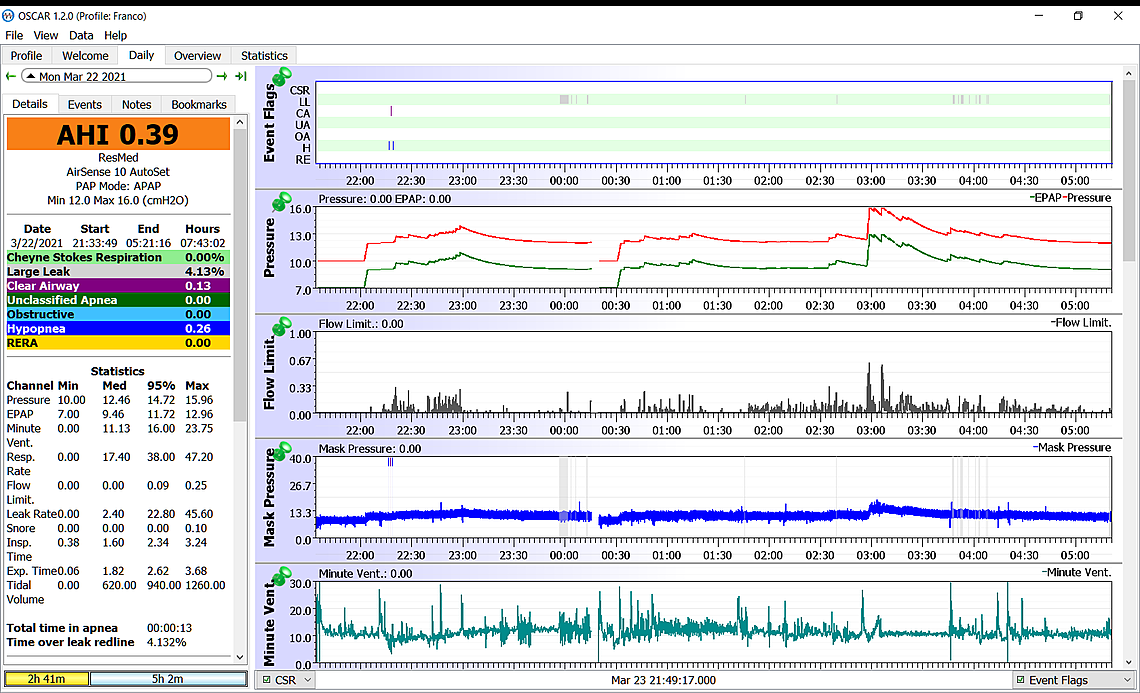
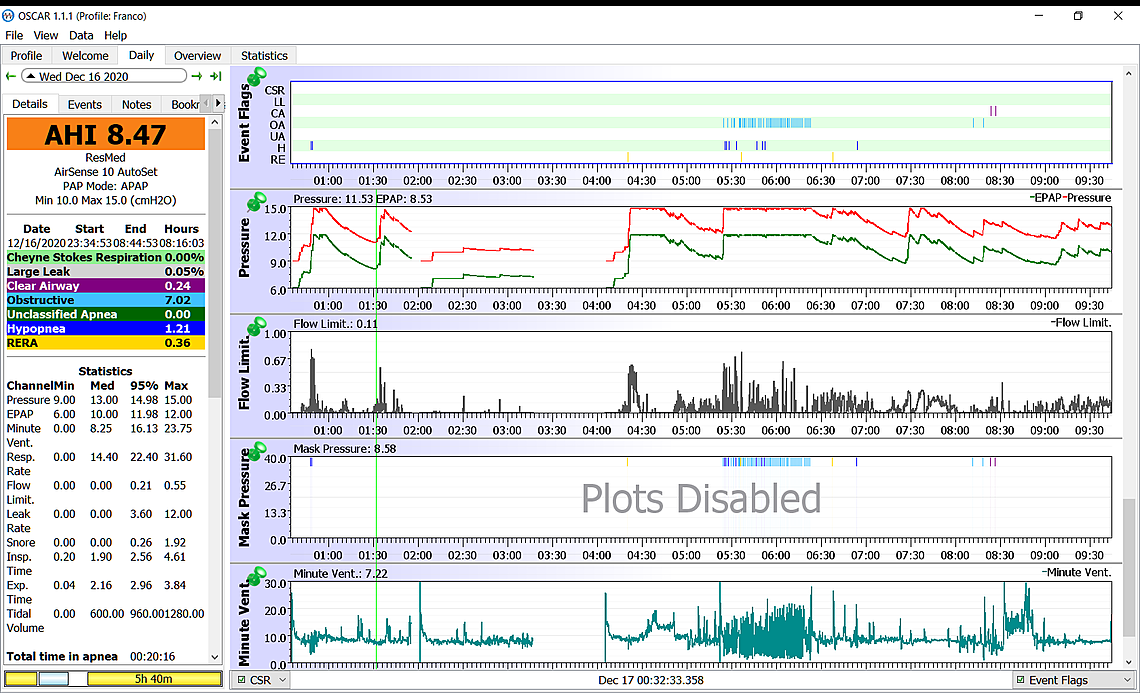
The report of 12/22 , which I will attach as soon as I know how to do it, shows for example 8.47 AHI’s, of which 7.02 ( practically 90%) are OA’s.
Considering the TTIA for the night ( about 20:min), each OA had a duration of 2.85 min. A lot! .
Of course, I didn’t stop breathing foe almost 3 min, or I’d be dead, but 20 min. of OA’s events shouldn’t perhaps be underestimated. This may be why my doctor has decided to increase the pressure.
3.I’d also like to have your take about the possible connection between sleep apnea and cardiac arrythmias. Can sleep apnea cause arrythmias?.
Two years ago, before being treated for Sleep Apnea, I had an episode of Afib, when I was about to begin my usual 6 km running session . I am 79 and it was the 1st time. The cardiologist put me on betablocker ( Metaprolol) as a precaution, but I had a 2nd episode a few days ago, with the pulse briefly shooting up to 160 bpm, with absolutely no discomfort, though.
I spoke to the doctor again. In the meantime my heart had gone back to normal, except that I have a lingering arrhythmia, with the pulse fluctuating between 90-110 bpm ( it usually is 60 bpm at rest ) , It doesn’t go away. I don’t even feel it and I can detect it only with the cardio watch, but it is still there.
If it it doesn’t go away, I’ll speak to my doctor again, but I wonder if arrythmias are an expected… byproduct of Sleep Apnea.
Thanks for your input, as usual
Ittiandro